Introduction
Mirror therapy is a type of motor imagery whereby the patient moves his unaffected limb while watching the movement in a mirror; this in turn sends a visual stimulus to the brain to promote movement in the affected limb. Some of the effects of mirror therapy on the brain have already been demonstrated. A crossover study on healthy individuals by Garry, Loftus & Summers (2004) showed that viewing the mirror image of an individual’s active hand increased the excitability of neurons in the ipsilateral primary motor cortex significantly more than viewing the inactive hand directly (no mirror). The study also found a trend toward significance in favour of viewing a mirror image of the active hand compared to viewing the active hand directly (no mirror).
There is a growing body of evidence regarding the use of mirror therapy on the upper extremity following stroke. Please also see our Mirror Therapy – Lower Extremity module for studies that have investigated the use of mirror therapy with the lower limbs.
Patient/Family Information
What is mirror therapy?
Mirror therapy is a specific therapy designed to strengthen arms and hands weakened by a stroke. In mirror therapy, we use movements of the stronger hand and arm to “trick our brain” into thinking that the weaker arm is moving. Researchers have shown that this “tricking of the brain” actually works – the brain areas responsible for making the weaker arm move become stimulated. There is also some new work being done using mirror therapy on the leg (see photographs – under section – How often do I need to practice?)
How do I set up mirror therapy at home?
You start by placing a solid stand-alone mirror on a table lengthwise in front of you. NOTE: You should sit in a sturdy chair while doing this activity. Place both your arms on the table one on either side of the mirror. The mirror side (where you can see the reflection of your arm) is placed so that you see your stronger arm. It is important that the mirror is large enough so that you can see your whole arm and hand in it. You should not look at your weaker hand and arm – only focus on looking into the mirror. Now move your stronger hand while you watch the mirror. The image that you see in the mirror will make it seem like your weak hand is moving. This information on arm movement is sent to your brain that is then “tricked” into thinking that your weaker arm is moving.


Will it be of benefit to me?
Mirror therapy is especially useful for people who have very little movement of their arm and hand after a stroke. The research on how well this intervention works is still quite new. There is some encouraging evidence that suggests that by using mirror therapy, the part of your brain that is damaged is stimulated, encouraging recovery. In fact, research has shown that some patients experience greater improvements in movement when they participate in mirror therapy in addition to their regular therapy, instead of just regular therapy alone. More research in the future will give us more information on just how beneficial mirror therapy is after a stroke.
Are there any risks to me?
There are no specific risks involved in participating in mirror therapy. It is important to use a non-breakable mirror just in case it falls over. It is also important to work in a seated position so that you can focus on your arm and hand without having to think about your balance and standing safety.
Mirror therapy is actually quite easy to do at home and many people find it a fun way of having additional therapy for their hand and arm.
Do I need any special equipment?
While specialized mirror boxes are available for purchase, using a sturdy table-sized mirror with a good solid stand works just as well.
How often do I need to practice?
There is no standardized protocol for mirror therapy. You should start with whatever amount of time you can tolerate and enjoy, and then gradually work up to a full series of movements and activities.


How do I begin?
Your rehabilitation therapist should be able to provide you with a program that will meet your individual needs. She or he can guide you as to:
- how many times a week you should do mirror therapy,
- what specific activities and movements you should do,
- what activities you should not do,
- how long each mirror therapy session should be,
- how to change activities as your hand and arm get stronger.
Clinician Information
Note: When reviewing the findings, it is important to note that they are always made according to randomized clinical trial (RCT) criteria – specifically as compared to a control group. To clarify, if a treatment is “effective” it implies that it is more effective than the control treatment to which it was compared. Non-randomized studies are no longer included when there is sufficient research to indicate strong evidence (level 1a) for an outcome.
Thirty-five studies (18 high quality RCTs, 14 fair quality RCTs, two poor quality RCTs and one non-randomized study) have investigated the effect of mirror therapy post-stroke. Of these, just three studies (one high quality RCT, one fair quality RCT and one non-randomized study) were conducted specifically with patients in the acute phase of stroke recovery, whereas the majority of studies were conducted with patients in the subacute or chronic phases of recovery. Across studies, outcomes included functional independence, dexterity, grip strength and hand function, upper extremity kinematics, sensory function, motor function and activity, pain, range of motion, and unilateral spatial neglect.
Results from this StrokEngine review showed strong evidence (level 1a) to support the use of mirror therapy to improve unilateral spatial neglect in the subacute phase of stroke recovery, and to improve upper extremity kinematics and motor function in the chronic phase of stroke recovery. Mirror therapy was comparable with other interventions for other outcomes. No adverse effects were reported.
Results Table
View results table
Outcomes
Acute Phase
Functional independence
Effective
2A
One fair quality RCT (Invernizzi et al., 2013) and one non-randomized study (Yeldan et al., 2015) investigated the effect of mirror therapy on functional independence in patients with acute stroke.
The fair quality RCT (Invernizzi et al., 2013) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Functional independence was measured by the Functional Independence Measure at post-treatment (4 weeks). There was a significant between-group difference, in favour of mirror therapy vs. sham mirror therapy.
The non-randomized study (Yeldan et al., 2015) assigned patients to receive mirror therapy or no mirror therapy; both groups received neurodevelopmental treatment. Functional independence was measured by the Barthel Index at post-treatment (3 weeks). No significant between-group difference was found.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is more effective than a comparison intervention (sham mirror therapy) for improving functional independence in patients with acute stroke.
Note: A non-randomized study found no difference between mirror therapy and no mirror therapy, when both patient groups also received neurodevelopmental treatment.
Motor function
Effective
2A
One fair quality RCT (Invernizzi et al., 2013) and one non-randomized study (Yeldan et al., 2015) investigated the effect of mirror therapy on upper extremity motor function in patients with acute stroke.
The fair quality RCT (Invernizzi et al., 2013) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the Action Research Arm Test at post-treatment (4 weeks). There was a significant between-group difference, in favour of mirror therapy vs. sham mirror therapy.
The non-randomized study (Yeldan et al., 2015) assigned patients to receive mirror therapy or no mirror therapy; both groups received neurodevelopmental treatment. Upper extremity motor function was measured by the Fugl-Meyer Assessment – Upper Extremity, and Stroke Upper Limb Capacity Scale at post-treatment (3 weeks). No significant between-group differences on any of the measures were found.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is more effective than a comparison intervention (sham mirror therapy) for improving upper extremity motor function in patients with acute stroke.
Note: A non-randomized study found no difference between mirror therapy and no mirror therapy, when both patient groups also received neurodevelopmental treatment.
Sensory integration
Not effective
2b
One non-randomized study (Yeldan et al., 2015) investigated the effect of mirror therapy on upper extremity sensory integration in patients with acute stroke. This study assigned patients to receive mirror therapy or no mirror therapy; both groups received neurodevelopmental treatment. Somatosensory perception was measured by the Ayres Southern Californian Sensory Integration Tests (Finger identification, Right-left discrimination items) at post-treatment (3 weeks). No significant between-group differences on any of the measures were found.
Conclusion: There is limited evidence (Level 2b) from one non-randomized study that mirror therapy is not more effective than no mirror therapy for improving somatosensory perception in patients with acute stroke.
One fair quality RCT (Invernizzi et al., 2013) and one non-randomized study (Yeldan et al., 2015) investigated the effect of mirror therapy on upper extremity strength in patients with acute stroke.
The fair quality RCT (Invernizzi et al., 2013) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity strength was measured by the Motricity Index at post-treatment (4 weeks). There was a significant between-group difference, in favour of mirror therapy vs. sham mirror therapy.
The non-randomized study (Yeldan et al., 2015) assigned patients to receive mirror therapy or no mirror therapy; both groups received neurodevelopmental treatment. Upper extremity strength was measured by the Motricity Index at post-treatment (3 weeks). No significant between-group difference was found.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is more effective than a comparison intervention (sham mirror therapy) for improving upper extremity strength in patients with acute stroke.
Note: A non-randomized study found no difference between mirror therapy and no mirror therapy, when both patient groups also received neurodevelopmental treatment.
Unilateral spatial neglect
Effective
1B
One high quality RCT (Pandian et al., 2014) investigated the effect of mirror therapy on unilateral spatial neglect in patients with acute stroke. This high quality RCT randomized patients to receive mirror therapy or sham mirror therapy. Unilateral spatial neglect was measured by the Star Cancellation Test, Line Bisection Test and Picture Identification Task at post-treatment (1 month) and follow-up (3 months, 6 months). There were significant between-group differences in all measures at all time points, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is more effective than a comparison intervention (sham mirror therapy) for improving unilateral spatial neglect in patients with acute stroke.
Subacute Phase
Two high quality RCTs (Kim, Lee & Song, 2014; Samuelkamaleshkumar et al., 2014) investigated the effect of mirror therapy on dexterity in patients with subacute stroke.
The first high quality RCT (Kim, Lee & Song, 2014) randomized patients to receive mirror therapy and functional electrical stimulation (FES) or sham mirror therapy and FES; both groups received conventional rehabilitation. Dexterity was measured by the Box and Block Test at post-treatment (4 weeks). No significant between-group difference was found.
The second high quality RCT (Samuelkamaleshkumar et al., 2014) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Dexterity was measured by the Box and Block Test at post-treatment (3 weeks). A significant between-group difference was found, in favour of mirror therapy vs. no mirror therapy.
Conclusion: Conflicting evidence (Level 4) between two high quality RCTs was found regarding the effect of mirror therapy on dexterity in patients with subacute stroke . These evidence indicate that mirror therapy is not more effective than simulated mirror therapy and functional electrical stimulation, but more effective than no mirror therapy.
Functional independence
Not effective
1A
Three high quality RCTs (Dohle et al., 2009; Thieme et al., 2012; Lim et al., 2016) and two fair quality RCTs (Radajewska et al., 2013, 2017; Gurbuz et al., 2016) investigated the effect of mirror therapy on functional independence in patients with subacute stroke.
The first high quality RCT (Dohle et al., 2009) randomized patients to receive mirror therapy or upper extremity training while watching the affected limb. Functional independence was measured by the Functional Independence Measure (FIM – Motor score) at post-treatment (6 weeks). No significant between-group difference was found.
The second high quality RCT (Thieme et al., 2012) randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Functional independence was measured by the Barthel Index (BI) at post-treatment (5 weeks). No significant between-group differences were found.
The third high quality RCT (Lim et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy. Functional independence was measured by the modified BI at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
The first fair quality RCT (Radajewska et al., 2013, 2017) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional stroke rehabilitation. Functional independence was measured by the Functional Index ‘Repty’ at post-treatment (3 weeks). No significant between-group difference was found.
The second fair quality RCT (Gurbuz et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy. Functional independence was measured by the FIM at post-treatment (4 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs and two fair quality RCTs that mirror therapy is not more effective than comparison interventions (upper extremity training while watching the affected limb, sham group mirror therapy, no mirror therapy) in improving functional independence in patients with subacute stroke.
Note: However, a third high quality RCT found that mirror therapy was more effective than sham mirror therapy.
Motor activity
Effective
1b
One high quality RCT (Cacchio et al., 2009a) investigated the effect of mirror therapy on upper limb motor activity in patients with subacute stroke. This high quality RCT randomized patients with subacute stroke and Complex Regional Pain Syndrome type 1 to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity motor activity was measured by the Motor Activity Log – Quality of Movement score at post-treatment (4 weeks) and follow-up (6 months). A significant between-group difference was found at both time points, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is more effective than a comparison intervention (sham mirror therapy) for improving upper extremity motor activity in patients with subacute stroke.
Motor function
Conflicting
4
Six high quality RCTs (Cacchio et al., 2009a; Dohle et al., 2009; Thieme et al., 2012; Kim, Lee & Song, 2014; Samuelkamaleshkumar et al., 2014; Lim et al., 2016) and eight fair quality RCTs (Yun et al., 2011; Lee, Cho & Song, 2012; Bae, Jeong & Kim, 2012; Radajewska et al., 2013, 2017; Mirela et al., 2015; Nagapattinam et al., 2015; Rehani, kumari & Midha, 2015; Gurbuz et al., 2016) investigated the effect of mirror therapy on upper extremity motor function in patients with subacute stroke.
The first high quality RCT (Cacchio et al., 2009a) randomized patients with subacute stroke and Complex Regional Pain Syndrome type 1 to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the Wolf Motor Function Test – Functional Ability and Performance Time (WMFT-FA; WMFT-PT) at post-treatment (4 weeks) and follow-up (6 months). Significant between-group differences were found on both measures and at both time points, in favour of mirror therapy vs. sham mirror therapy.
The second high quality RCT (Dohle et al., 2009) randomized patients to receive mirror therapy or upper extremity training while watching the affected limb. Upper extremity motor function was measured by the Action Research Arm Test (ARAT – Grasp, Grip, Pinch, Gross movement scores) and the Fugl-Meyer Assessment (FMA – Proximal arm, Hand, Finger scores) at post-treatment (6 weeks). No significant between-group differences were found.
Note: However, in a subgroup of patients with distal plegia, a significant difference was seen in distal function (FMA – Finger score), in favour of mirror therapy vs. sham mirror therapy.
The third high quality RCT (Thieme et al., 2012) randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Upper extremity motor function was measured by the ARAT and the FMA (Motor score) at post-treatment (5 weeks). No significant between-group differences on any of the measures were found.
The fourth high quality RCT (Kim, Lee & Song, 2014) randomized patients to receive mirror therapy and functional electrical stimulation (FES) or sham mirror therapy and FES; both groups received conventional rehabilitation. Upper extremity motor function was measured by the FMA (Shoulder/elbow/forearm, Wrist, Hand, Coordination subtests) and the Manual Function Test (MFT – Shoulder, Hand subtests) at post-treatment (4 weeks). Significant between-group differences in measures of distal function (FMA – Wrist, Hand subtests; MFT – Hand subtest) were seen, in favour of mirror therapy + FES vs. sham mirror therapy + FES.
The fifth high quality RCT (Samuelkamaleshkumar et al., 2014) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the FMA – Upper Extremity (FMA-UE) at post-treatment (3 weeks). A significant between-group difference was found, in favour of mirror therapy vs. no mirror therapy.
The sixth high quality RCT (Lim et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy. Upper extremity motor function was measured by the FMA at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
The first fair quality RCT (Yun et al., 2011) randomized patients to receive mirror therapy + neuromuscular electrical stimulation (NMES), mirror therapy, or NMES. Upper extremity motor function was measured by the FMA (Wrist, Hand, Coordination, combined scores) at post-treatment (3 weeks). There was no significant difference between mirror therapy vs. NMES.
Note: There were significant between-group differences in favour of mirror therapy + NMES vs. mirror therapy alone or NMES alone.
The second fair quality RCT (Lee, Cho & Song, 2012) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the FMA (Shoulder/elbow/forearm, Wrist, Hand, Coordination subtests) and the MFT (Upper limb, Hand subtests) at post-treatment (4 weeks). Significant between-group differences were found for most measures (FMA – Shoulder/elbow/forearm, Wrist, Hand subtests; MFT – Upper limb, Hand subtests), in favour of mirror therapy vs. no mirror therapy.
The third fair quality RCT (Bae, Jeong & Kim, 2012) randomized patients to receive mirror therapy or unilateral upper limb exercises while watching the non-paretic limb; both groups received conventional rehabilitation. Upper extremity motor function was measured by the MFT at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. unilateral upper limb exercises.
The fourth fair quality RCT (Radajewska et al., 2013, 2017) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional stroke rehabilitation. Upper extremity motor function was measured by the Frenchay Arm Test and Motor Status Score at post-treatment (3 weeks). A significant between-group difference in one measure of upper extremity motor function (Frenchay Arm Test) was found, in favour of mirror therapy vs. no mirror therapy.
The fifth fair quality RCT (Mirela et al., 2015) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the FMA-UE at post-treatment (6 weeks). A significant between-group difference was found, in favour of mirror therapy vs. no mirror therapy.
The sixth fair quality RCT (Nagapattinam et al., 2015) randomized patients to receive mirror therapy, FES, or mirror therapy + FES. Upper extremity motor function was measured by the ARAT (Grasp, Grip, Pinch, Gross movement, Total scores) at post-treatment (2 weeks). No significant between-group differences were found.
The seventh fair quality RCT (Rehani, kumari & Midha, 2015) randomized patients to receive mirror therapy or a Motor Relearning Principles exercise program; both groups received conventional physiotherapy. Upper extremity motor function was measured using the Chedoke Arm and Hand Activity Inventory at post-treatment (4 weeks). No significant between-group difference was found.
The eight fair quality RCT (Gurbuz et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy. Upper extremity motor function was measured by the FMA-UE at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is conflicting evidence (level 4) regarding the effect of mirror therapy on upper extremity motor function in patients with subacute stroke. Three high quality RCTs and five fair quality RCTs found that mirror therapy was more effective than no mirror therapy or comparison interventions (sham mirror therapy and unilateral upper limb exercises); however, two high quality RCTs and three fair quality RCTs found no difference between mirror therapy and comparison interventions (upper extremity training, sham group mirror therapy, neuromuscular electrical stimulation, functional electrical stimulation or Motor Relearning Principles exercise program).
Note: A high quality RCT found benefits were localised to distal function when mirror therapy was combined with FES. Another high quality RCT saw a significant difference in distal function of patients with distal plegia, in favour of mirror therapy vs. sham mirror therapy.
Motor recovery
Conflicting
4
Three high quality RCTs (Kim, Lee & Song, 2014; Samuelkamaleshkumar et al., 2014; Lim et al., 2016) and three fair quality RCTs (Lee, Cho & Song, 2012; Mirela et al., 2015; Gurbuz et al., 2016) investigated the effect of mirror therapy on upper extremity motor recovery in patients with subacute stroke.
The first high quality RCT (Kim, Lee & Song, 2014) randomized patients to receive mirror therapy and functional electrical stimulation (FES) or sham mirror therapy and FES; both groups received conventional rehabilitation. Upper extremity motor recovery was measured by Brunnstrom stages of motor recovery (Upper extremity, Hand scores) at post-treatment (4 weeks). A significant between-group difference in distal recovery (Hand score) was seen, in favour of mirror therapy + FES vs. sham mirror therapy + FES.
The second high quality RCT (Samuelkamaleshkumar et al., 2014) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor recovery was measured by Brunnstrom stages of motor recovery (Upper extremity, Hand scores) at post-treatment (3 weeks). Significant between-group differences were found in proximal and distal recovery, in favour of mirror therapy vs. no mirror therapy.
The third high quality RCT (Lim et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy. Upper extremity motor recovery was measured by Brunnstrom stages of motor recovery (Upper extremity, Hand scores) at post-treatment (4 weeks No significant between-group differences on any of the measures were found.
The first fair quality RCT (Lee, Cho & Song, 2012) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor recovery was measured by Brunnstrom stages of motor recovery (Upper extremity, Hand scores) at post-treatment (4 weeks). Significant between-group differences were found in proximal and distal recovery, in favour of mirror therapy vs. no mirror therapy.
The second fair quality RCT (Mirela et al., 2015) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor recovery was measured by Brunnstrom stages of motor recovery at post-treatment (6 weeks). No significant between-group difference was found.
The third fair quality RCT (Gurbuz et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Motor recovery was measured by Brunnstrom stages of motor recovery (Upper extremity, Hand scores) at post-treatment (4 weeks). No significant between-group differences on any of the measures were found.
Conclusion: There is conflicting evidence (Level 4) regarding the effect of mirror therapy on upper extremity motor recovery in patients with subacute stroke: One high quality RCT and one fair quality RCT found that mirror therapy was more effective than no mirror therapy, whereas one high quality RCT and two fair quality RCTs found no difference in outcomes between mirror therapy and sham/no mirror therapy.
Note: A third high quality RCT found that benefits were localised to distal motor recovery when mirror therapy was combined with FES.
Muscle power
Not effective
2a
One fair quality RCT (Yun et al., 2011) investigated the effect of mirror therapy on upper extremity muscle power in patients with subacute stroke. This fair quality RCT randomized patients to receive mirror therapy + neuromuscular electrical stimulation (NMES), mirror therapy, or NMES. Upper extremity muscle power (hand flexion/extension, wrist flexion/extension) was measured by manual muscle testing at post-treatment (3 weeks). There was no significant difference between mirror therapy and NMES.
Note: There were significant between-group differences in hand extension power only, in favour of mirror therapy + NMES vs. mirror therapy alone or NMES alone.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is not more effective than a comparison intervention (neuromuscular electrical stimulation) for improving muscle power in patients with subacute stroke.
Three high quality RCTs (Cacchio et al., 2009a; Dohle et al., 2009; Thieme et al., 2012) investigated the effect of mirror therapy on upper limb pain in patients with subacute stroke.
The first high quality RCT (Cacchio et al., 2009a) randomized patients with subacute stroke and Complex Regional Pain Syndrome type 1 to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity pain (at rest, on movement) and tactile allodynia were measured by visual analogue scale at post-treatment (4 weeks) and follow-up (6 months). Significant between-group differences in all measures were found at both time points, in favour of mirror therapy vs. sham mirror therapy.
The second high quality RCT (Dohle et al., 2009) randomized patients to receive mirror therapy or upper extremity training while watching the affected limb. Pain was measured by the Fugl-Meyer Assessment of Sensorimotor Recovery After Stroke (FMA – Pain score) at post-treatment (6 weeks). No significant between-group difference was found.
The third high quality RCT (Thieme et al., 2012) randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Upper extremity pain was measured by the FMA (Pain score) at post-treatment (5 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is not more effective than comparison interventions (upper extremity training while watching the affected limb, sham group mirror therapy) for reducing upper limb pain in patients with subacute stroke.
Note: However, one high quality RCT found that mirror therapy was more beneficial than sham mirror therapy for reducing pain and tactile allodynia in patients with subacute stroke and Complex Regional Pain Syndrome type 1, when measured using a visual analogue scale.
Range of motion
Not effective
1A
Two high quality RCTs (Dohle et al., 2009; Thieme et al., 2012) investigated the effect of mirror therapy on upper extremity range of motion (ROM) in patients with subacute stroke.
The first high quality RCT (Dohle et al., 2009) randomized patients to receive mirror therapy or upper extremity training while watching the affected limb. Upper extremity ROM was measured by the Fugl-Meyer Assessment of Sensorimotor Recovery After Stroke (FMA – ROM score) at post-treatment (6 weeks). No significant between-group difference was found.
The second high quality RCT (Thieme et al., 2012) randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Upper extremity ROM was measured by the FMA (ROM score) at post-treatment (5 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is not more effective than comparison interventions (upper extremity training while watching the affected limb or sham group mirror therapy) for improving upper extremity range of motion in patients with subacute stroke.
Sensory function
Not effective
1A
Two high quality RCTs (Dohle et al., 2009; Thieme et al., 2012) investigated the effect of mirror therapy on upper limb sensorimotor function in patients with subacute stroke.
The first high quality RCT (Dohle et al., 2009) randomized patients to receive mirror therapy or upper extremity training while watching the affected limb. Upper extremity sensorimotor function was measured by the Fugl-Meyer Assessment of Sensorimotor Recovery After Stroke (FMA – Light touch, Proprioception scores) at post-treatment (6 weeks). A significant between-group difference in surface sensibility (FMA – Light touch) was found in favour of mirror therapy group vs. upper extremity training.
The second high quality RCT (Thieme et al., 2012) randomized patients with subacute stroke to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Upper extremity sensorimotor function was measured by the FMA (Sensory score) at post-treatment (5 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is not more effective than comparison interventions (upper extremity training, sham group mirror therapy) for improving upper extremity sensory function (proprioception only) in patients with subacute stroke.
Note: There was conflicting evidence between the two studies regarding the effect of mirror therapy on light touch – mirror therapy was more effective than upper extremity training but was no more effective than sham group mirror therapy.
Spasticity
Not effective
1A
Two high quality RCTs (Thieme et al., 2012; Samuelkamaleshkumar et al., 2014) and two fair quality RCTs (Yun et al., 2011; Mirela et al., 2015) investigated the effect of mirror therapy on upper extremity spasticity in patients with subacute stroke.
The first high quality RCT (Thieme et al., 2012) randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Upper extremity spasticity was measured by the Modified Ashworth Scale (MAS – Finger flexors, Wrist flexors) at post-treatment (5 weeks). No significant differences between mirror therapy vs. sham group mirror therapy were found.
Note: A significant between-group difference in resistance to passive movement of finger flexors was found, in favour of individual mirror therapy vs. group mirror therapy.
The second high quality RCT (Samuelkamaleshkumar et al., 2014) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity spasticity was measured by the MAS at post-treatment (3 weeks). No significant between-group difference was found.
The first fair quality RCT (Yun et al., 2011) randomized patients to receive mirror therapy + neuromuscular electrical stimulation (NMES), mirror therapy, or NMES. Upper extremity spasticity was measured by the MAS at post-treatment (3 weeks). No significant between-group difference was found.
The second fair quality RCT (Mirela et al., 2015) randomized patients to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity spasticity was measured by the MAS (Shoulder, Elbow, Wrist scores) and the Bhakta Test (Finger flexion scale) at post-treatment (6 weeks). Significant between-group differences in distal spasticity (MAS – Wrist; Bhakta Test – Finger flexion scale) were found, in favour of mirror therapy vs. no mirror therapy.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs and one fair quality RCT that mirror therapy is not more effective than comparison interventions (group sham mirror therapy, no mirror therapy, neuromuscular electrical stimulation) for reducing upper extremity spasticity in patients with subacute stroke.
Note: One fair quality RCT found that mirror therapy was more effective than no mirror therapy for reducing distal spasticity.
Stroke outcomes
Not effective
1B
One high quality RCT (Thieme et al., 2012) investigated the effect of mirror therapy on stroke outcomes in patients with subacute stroke. This high quality RCT randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Stroke outcomes were measured by the Stroke Impact Scale at post-treatment (5 weeks). There was no significant difference between groups.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is not more effective than a comparison intervention (sham group mirror therapy) for improving stroke outcomes in patients with subacute stroke.
Unilateral spatial neglect
Effective
1A
Two high quality RCTs (Dohle et al., 2009; Thieme et al., 2012) investigated the effect of mirror therapy on unilateral spatial neglect in patients with subacute stroke.
The first high quality RCT (Dohle et al., 2009) randomized patients to receive mirror therapy or upper extremity training while watching the affected limb. Unilateral spatial neglect was measured by a non-validated 5-point rating scale derived from the Behavioural Inattention Test and the Tests of Attentional Performance at post-treatment (6 weeks). A significant between-group difference was found, in favour of mirror therapy vs. upper extremity training watching the affected limb.
The second high quality RCT (Thieme et al., 2012) randomized patients to receive individual mirror therapy, group mirror therapy, or sham group mirror therapy. Unilateral spatial neglect was measured by the Star Cancellation Test at post-treatment (5 weeks). A significant between-group difference was found, in favour of individual mirror therapy vs. sham group mirror therapy.
Note: There were no significant differences between individual vs. group mirror therapy, nor between group mirror therapy vs. sham group mirror therapy.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is more effective than comparison interventions (upper extremity training while watching the affected limb, group sham mirror therapy) for improving unilateral spatial neglect in patients with subacute stroke.
Chronic phase
Two high quality RCTs (Ji, Cha & Kim, 2014; Lin et al., 2014), two fair quality RCTs (Cho & Cha, 2015; Kim et al., 2016) and one poor quality RCT (Park et al., 2015a) examined the effect of mirror therapy on dexterity in patients with chronic stroke.
The first high quality RCT (Ji, Cha & Kim, 2014) randomized patients to receive mirror therapy, mirror therapy + repetitive Transcranial Magnetic Stimulation (rTMS), or sham mirror therapy. Dexterity was measured by the Box and Block Test (BBT) at post-treatment (6 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
Note: A significant between-group difference was also found in favour of mirror therapy + rTMS vs. mirror therapy.
The second high quality RCT (Lin et al., 2014) randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Manual dexterity was measured by the BBT at post-treatment (4 weeks). A significant between-group difference was found, in favour of task-oriented training vs. mirror therapy.
Note: A significant between-group difference was found in favour of mirror therapy + electrical stimulation vs. mirror therapy. There were no differences between mirror therapy + electrical stimulation vs. task-oriented training.
The first fair quality RCT (Cho & Cha, 2015) randomized patients to receive mirror therapy or sham mirror therapy; both groups received transcranial direct current stimulation. Dexterity was measured by the BBT at post-treatment (6 weeks). There was a significant between-group difference in favour of mirror therapy vs. sham mirror therapy.
The second fair quality RCT (Kim et al., 2016) randomized patients to receive mirror therapy or conventional rehabilitation. Dexterity was measured by the BBT at post-treatment (4 weeks). There was a significant between-group difference, favouring mirror therapy vs. conventional rehabilitation.
The poor quality RCT (Park et al., 2015a) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Dexterity was measured by the BBT at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is conflicting evidence (Level 4) regarding the effect of mirror therapy on dexterity in the chronic phase of stroke recovery. While one high quality RCT, two fair quality RCTs and one poor quality RCT found that mirror therapy was more effective than comparison interventions (sham mirror therapy, conventional rehabilitation), a second high quality RCTfound that mirror therapy was not more effective than task-oriented training.
Note: Two high quality RCTs found that mirror therapy and repetitive Transcranial Magnetic Stimulation / electrical stimulation are more effective than mirror therapy alone for improving dexterity in the chronic phase of stroke recovery.
Functional independence
Effective
2a
Two fair quality RCTs (Park et al., 2015b; Kim et al., 2016) and one poor quality RCT (Park et al., 2015a) investigated the effect of mirror therapy on functional independence in patients with chronic stroke.
The first fair quality RCT (Park et al., 2015b) randomized patients to receive mirror therapy or sham mirror therapy. Functional independence was measured by the Functional Independence Measure (FIM) at baseline and at post-treatment (6 weeks). A significant between-group difference in change scores from baseline to post-treatment was found, in favour of mirror therapy vs. sham mirror therapy.
The second fair quality RCT (Kim et al., 2016) randomized patients to receive mirror therapy or conventional rehabilitation. Functional independence was measured by the FIM at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. conventional rehabilitation.
The poor quality RCT (Park et al., 2015a) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Functional independence was measured by the Functional Independence Measure (Total, Self-care, Sphincter control, Transfer, Locomotion, Communication, Social cognition scores) at post-treatment (4 weeks). Significant between-group differences were found (FIM: Total, Self-care scores), in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is limited evidence (Level 2a) from two fair quality RCTs and one poor quality RCT that mirror therapy is more effective than comparison interventions (sham mirror therapy, conventional rehabilitation) for improving functional independence in patients with chronic stroke.
Grip strength
Not effective
1b
One high quality RCT (Michielsen et al., 2010) and one fair quality RCT (Cho & Cha, 2015) investigated the effect of mirror therapy on grip strength in patients with chronic stroke.
The high quality RCT (Michielsen et al., 2010) randomized patients to receive mirror therapy or bimanual exercises with sight of both hands. Grip force was measured by Jamar handheld dynamometer at post-treatment (6 weeks) and follow-up (6 months). No significant between-group difference was found at either time point.
The fair quality RCT (Cho & Cha, 2015) randomized patients to receive mirror therapy or sham mirror therapy; both groups received transcranial direct current stimulation. Grip strength was measured by Jamar handheld dynamometer at post-treatment (6 weeks). There was a significant between-group difference, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is not more effective than a comparison intervention (bimanual exercises with sight of both hands) in improving grip strength among patients with chronic stroke.
Note: However, a fair quality RCT found that mirror therapy was more effective than sham mirror therapy. In this study, participants in the comparison group performed bilateral exercises without vision of the non-paretic arm; in the high quality RCT participants completed bilateral exercises with sight of both hands. Differences in treatment regime and intensity may also account for discrepancies between studies.
Hand function
Not effective
2a
One fair quality RCT (Cho & Cha, 2015) examined the effect of mirror therapy on hand function in patients with chronic stroke. This fair quality RCT randomized patients to receive mirror therapy or sham mirror therapy; both groups received transcranial direct current stimulation. Hand function was measured by the Jebsen Taylor Test of Hand Function at post-treatment (6 weeks). No significant between-group difference was found.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is not more effective than a comparison therapy (sham mirror therapy) for improving hand function among patients with chronic stroke.
Two high quality RCTs (Wu et al., 2013; Lin et al., 2014) investigated the effect of mirror therapy on upper extremity kinematics in patients with chronic stroke.
The first high quality RCT (Wu et al., 2013) randomized patients to receive mirror therapy or task-oriented training. Upper extremity kinematics (reaction time, normalized movement time, normalized total displacement, normalized shoulder flexion, normalized elbow extension, maximum shoulder abduction, maximum shoulder/elbow cross-correlation) were measured at post-treatment (4 weeks). Significant between-group differences in some kinematic variables (reaction time, normalized total displacement, maximum shoulder-elbow cross-correlation) were found, in favour of mirror therapy vs. task-oriented training.
The second high quality RCT (Lin et al., 2014) randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Upper extremity kinematics (wrist normalized movement time, wrist normalized movement units, normalized shoulder flexion, normalized elbow extension, maximum shoulder abduction) were measured at post-treatment (4 weeks). A significant between-group difference in maximum shoulder abduction was found in favour of mirror therapy vs. task-oriented training. Conversely, a significant difference in normalized shoulder flexion was found in favour of task-oriented training vs. mirror therapy.
Note: A significant between-group difference in maximum shoulder abduction was found in favour of mirror therapy + electrical stimulation vs. task-oriented training.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is more effective than a comparison intervention (task-oriented training) for improving some kinematic variables among patients with chronic stroke.
One high quality RCT (Lin et al., 2014) investigated the effect of mirror therapy on mobility in patients with chronic stroke. This high quality RCT randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Mobility was measured by the 10-Minute Walk Test (velocity, stride length) performed at two speeds (self-paced, as quick as possible) at post-treatment (4 weeks). Significant between-group differences in most measures of mobility (self-paced – velocity, stride length; as quick as possible – velocity) were found, in favour of task-oriented training vs. mirror therapy.
Note: There were significant between-group differences in mobility (self-paced – velocity, stride length; as quick as possible – velocity), in favour of mirror therapy + electrical stimulation vs. mirror therapy. There were no differences between mirror therapy + electrical stimulation vs. task-oriented training.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that upper extremity mirror therapy is not more effective than a comparison intervention (task-oriented training) for improving mobility in patients with chronic stroke.
Motor activity
Not effective
1A
Three high quality RCTs (Wu et al., 2013; Lin et al., 2014; Rodrigues et al., 2016) investigated the effect of mirror therapy on upper extremity motor activity in patients with chronic stroke.
The first high quality RCT (Wu et al., 2013) randomized patients to receive mirror therapy or task-oriented training. Upper extremity motor activity was measured by the Motor Activity Log – Amount of Use (MAL-AOU) and – Quality of Movement (MAL-QOM) subtests at post-treatment (4 weeks) and follow-up (6 months). There were no significant between-group differences at either time point.
The second high quality RCT (Lin et al., 2014) randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Upper extremity motor activity was measured by the MAL-AOU and MAL-QOM at post-treatment (4 weeks). There were no significant differences between groups.
The third high quality RCT (Rodrigues et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy watching the paretic upper limb. Upper extremity motor activity was measured by the Brazilian version of the TEMPA (Total, Unilateral, Bilateral scores) at post-treatment (4 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from three high quality RCTs that mirror therapy is not more effective than comparison interventions (task-oriented training, sham mirror therapy watching the paretic upper limb) for improving upper extremity motor activity in patients with chronic stroke.
Motor function
Effective
1A
Eight high quality RCTs (Michielsen et al., 2010; Wu et al., 2013; Ji, Cha & Kim, 2014; Lin et al., 2014; Arya et al., 2015; Colomer, Noe & Llorens, 2016; Rodrigues et al., 2016; Arya et al., 2018), four fair quality RCTs (Altschuler et al., 1999; Cho & Cha, 2015; Park et al., 2015b; Kim et al., 2016) and one poor quality RCT (Park et al., 2015a) investigated the effect of mirror therapy on upper extremity motor function in the chronic phase of stroke recovery.
The first high quality RCT (Michielsen et al., 2010) randomized patients to receive mirror therapy or bimanual exercise training with sight of both hands. Upper extremity motor function was measured by the Action Research Arm Test (ARAT) and the Fugl-Meyer Assessment (FMA) at post-treatment (6 weeks) and follow-up (6 months). A significant between-group difference in one measure (FMA) was found at post-treatment, in favour of mirror therapy vs. bimanual exercises. Results did not remain significant at follow-up.
The second high quality RCT (Wu et al., 2013) randomized patients to receive mirror therapy or task-oriented training. Upper extremity motor function was measured by the Fugl-Meyer Assessment – Upper Extremity (FMA-UE – Total, Proximal, Distal scores) at post-treatment (4 weeks). Significant between-group differences (FMA-UE – Total, Distal scores) were found, in favour of mirror therapy vs. task-oriented training.
The third high quality RCT (Ji, Cha & Kim, 2014) randomized patients to receive mirror therapy, mirror therapy + repetitive Transcranial Magnetic Stimulation (rTMS), or sham mirror therapy. Upper extremity motor function was measured by the FMA at post-treatment (6 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
Note: A significant between-group difference was also found in favour of mirror therapy + rTMS vs. mirror therapy.
The fourth high quality RCT (Lin et al., 2014) randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Upper extremity motor function was measured by the FMA at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. task-oriented training.
Note: There was also a significant between-group difference in favour of mirror therapy + electrical stimulation vs. task-oriented training. There were no significant differences between mirror therapy vs. mirror therapy + electrical stimulation.
The fifth high quality RCT (Arya et al., 2015) randomized patients to receive mirror therapy or conventional occupational therapy. Upper extremity motor function was measured using the FMA-UE, Upper arm (FMA-UA) and Wrist/hand (FMA-W/H) scores at post-treatment (8 weeks). Significant between-group differences in two measures (FMA-UE, FMA-W/H) were found, in favour of mirror therapy vs. conventional occupational therapy.
The sixth high quality RCT (Colomer, Noe & Llorens, 2016) randomized patients to receive mirror therapy or passive mobilisation of the upper extremity. Upper extremity motor function was measured by the Wolf Motor Function Test – Performance time (WMFT-PT) and Functional ability (WMFT-FA) scores and the FMA-UE at post-treatment (8 weeks). No significant between-group differences on any of the measures were found.
The seventh high quality RCT (Rodrigues et al., 2016) randomized patients to receive mirror therapy or sham mirror therapy watching the paretic upper limb. Upper extremity motor function was measured by the FMA-UE (Total, Proximal, Distal scores) at post-treatment (4 weeks). No significant between-group differences on any of the measures were found.
The eighth high quality RCT (Arya et al., 2018) randomized patients to receive mirror therapy or time-matched standard motor and sensory rehabilitation. Upper extremity motor function was measured using the FMA/WH subscore at post-treatment (6 weeks). A significant between-group difference was found, in favour of mirror therapy vs. standard motor and sensory rehabilitation.
The first fair quality crossover study (Altschuler et al., 1999) randomized patients to receive mirror therapy or bilateral exercises with view of the affected arm. Upper extremity motor function (speed, accuracy of cardinal movement) was measured using a 7-point Likert scale at mid-treatment (2 weeks), post-treatment (4 weeks) and follow-up (6 weeks, 8 weeks). Patients demonstrated better outcomes following mirror therapy than the comparison intervention at all time points.
Note: Statistical data were not provided.
The second fair quality RCT (Cho & Cha, 2015) randomized patients to receive mirror therapy or sham mirror therapy; both groups received transcranial direct current stimulation. Upper extremity motor function was measured by the FMA at post-treatment (6 weeks). No significant between-group difference was found.
The third fair quality RCT (Park et al., 2015b) randomized patients to receive mirror therapy or sham mirror therapy. Upper extremity motor function was measured by the Manual Function Test at post-treatment (6 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
The fourth fair quality RCT (Kim et al., 2016) randomized patients to receive mirror therapy or conventional rehabilitation. Upper extremity motor function was measured by the ARAT and the FMA at post-treatment (4 weeks). Significant between-group differences were found on both measures, favouring mirror therapy vs. conventional rehabilitation.
The poor quality RCT (Park et al., 2015a) randomized patients to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the FMA at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is strong evidence (Level 1a) from six high quality RCTs, two fair quality RCTs and one poor quality RCT that mirror therapy is more effective than comparison interventions (bimanual exercises with sight of both hands, task-oriented training, sham mirror therapy, conventional occupational therapy, standard motor and sensory rehabilitation or conventional rehabilitation) for improving upper extremity motor function in patients with chronic stroke. A third fair quality RCT also reported improved motor function following mirror therapy.
Note: However, two high quality RCTs and one fair quality RCT reported no significant difference between mirror therapy and comparison interventions (passive mobilisation, sham mirror therapy). Differences in outcome measures used, as well as the intensity and duration of interventions, may account for discrepancies in results among studies.
Two high quality RCTs (Cacchio et al., 2009b; Michielsen et al., 2010) have investigated the effect of mirror therapy on pain in patients with chronic stroke.
The first high quality RCT (Cacchio et al., 2009b) randomized patients with chronic stroke and Complex Regional Pain Syndrome type 1 to receive mirror therapy, sham mirror therapy or mental imagery. Pain was measured by visual analogue scale (VAS) at post-treatment (4 weeks). Significant between-group differences in pain on movement were found, in favour of mirror therapy vs. sham mirror therapy and mental imagery.
The second high quality RCT (Michielsen et al., 2010) randomized patients to receive mirror therapy or bimanual exercises with sight of both hands. Pain was measured by VAS at post-treatment (6 weeks) and follow-up (6 months). No significant between-group difference was found at either time point.
Conclusion: There is conflicting evidence (Level 4) between two high quality RCTs regarding the effect of mirror therapy on pain in patients with chronic stroke. One high quality RCT found that mirror therapy was more effective than comparison interventions (sham mirror therapy, mental imagery) for improving pain in patients with chronic stroke and Complex Regional Pain Syndrome type 1, whereas a second high quality RCT found that mirror therapy is not more effective than a comparison therapy (bimanual exercises with sight of both hands).
Quality of life
Not effective
1B
One high quality RCT (Michielsen et al., 2010) investigated the effect of mirror therapy on quality of life in patients with chronic stroke. This high quality RCT randomized patients to receive mirror therapy or bimanual exercises with sight of both hands. Quality of life was measured by the EuroQol-5D at post-treatment (6 weeks) and follow-up (6 months). No significant difference was found at either time point.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is not more effective than a comparison intervention (bimanual exercises with sight of both hands) for improving quality of life in patients with chronic stroke.
Range of motion
Insufficient evidence
5
One fair quality (Altschuler et al., 1999) investigated the effect of mirror therapy on upper extremity range of motion in patients with chronic stroke. This fair quality crossover study randomized patients to receive mirror therapy or bilateral exercises with view of the affected arm. Upper extremity range of motion was measured using a 7-point Likert scale at mid-treatment (2 weeks), post-treatment (4 weeks) and follow-up (6 weeks, 8 weeks). Patients demonstrated better range of motion following mirror therapy than the comparison intervention at all time points.
Note: Statistical data were not provided.
Conclusion: There is insufficient evidence (Level 5) regarding the effect of mirror therapy on range of motion in patients with chronic stroke. One fair quality RCT found improvements in range of motion following mirror therapy in comparison to bilateral exercises with view of the affected arm.
Self-perceived upper extremity function
Not effective
1a
Three high quality RCTs (Michielsen et al., 2010; Wu et al., 2013; Lin et al., 2014) investigated the effect of mirror therapy on self-perceived upper extremity function in patients with chronic stroke.
The first high quality RCT (Michielsen et al., 2010) randomized patients to receive mirror therapy or bimanual exercise training with sight of both hands. Self-perceived upper extremity function was measured by the ABILHAND at post-treatment (6 weeks) and follow-up (6 months). No significant between-group difference was found at either time point.
The second high quality RCT (Wu et al., 2013) randomized patients to receive mirror therapy or task-oriented training. Self-perceived upper extremity motor function was measured by the ABILHAND at post-treatment (4 weeks) and follow-up (6 months). No significant between-group difference was found at either time point.
The third high quality RCT (Lin et al., 2014) randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Self-report of upper extremity motor function was measured by the ABILHAND at post-treatment (4 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from three high quality RCTs that mirror therapy is not more effective than comparison interventions (bimanual exercises with sight of both hands, task-oriented training, mirror therapy + electrical stimulation) in improving self-perceived upper extremity function in patients with chronic stroke.
Sensory function
Not effective
1A
Three high quality RCTs (Wu et al., 2013; Colomer, Noe & Llorens, 2016; Arya et al., 2018) investigated the effect of mirror therapy on upper extremity sensory function in patients with chronic stroke.
The first high quality RCT (Wu et al., 2013) randomized patients to receive mirror therapy or task-oriented training. Upper extremity sensory function was measured by the revised Nottingham Sensory Assessment – Tactile subtest (Light touch, Temperature, Pinprick, Pressure, Tactile localization, Bilateral simultaneous touch, Tactile total score) at post-treatment (4 weeks). A significant between-group difference was found on only one measure of sensory function (Temperature), in favour of mirror therapy vs. task-oriented training.
The second high quality RCT (Colomer, Noe & Llorens, 2016) randomized patients to receive mirror therapy or passive mobilisation of the upper extremity. Upper extremity sensation was measured by the Nottingham Sensory Assessment – Tactile (Light touch, Pressure, Pinprick, Temperature, Tactile localisation, Bilateral simultaneous touch), Kinaesthetic and Stereognosis scores at post-treatment (8 weeks). A significant between-group difference was found on one measure of upper extremity sensation (Light touch), in favour of mirror therapy vs. passive mobilisation.
The third high quality RCT (Arya et al., 2018) randomized patients to receive mirror therapy or time-matched standard motor and sensory rehabilitation. Sensory function was measured at post-treatment (6 weeks) using the Semmes-Weinstein Monofilaments to assess cutaneous thresholds of the palm and fingers, and the 2-Point Discrimination Test to measure touch discrimination. No significant between-group difference in mean change in cutaneous thresholds for the affected fingers and palm were found. An increase in the number of positive responses for the finger quadrants and palm was found, in favour of mirror therapy vs. motor and sensory rehabilitation.
Note: A reliable assessment of touch discrimination was not achieved as only 26% of participants (n=17, 4 respectively) responded to touch discrimination testing on the affected side.
Conclusion: There is strong evidence (Level 1a) from three high quality RCTs that mirror therapy is not more effective than comparison interventions (task-oriented training, passive mobilisation or motor and sensory rehabilitation) for improving upper extremity sensory function in patients with chronic stroke.
Spasticity/tone
Not effective
1A
Two high quality RCTs (Michielsen et al., 2010; Lin et al., 2014) investigated the effect of mirror therapy on upper extremity spasticity in patients with chronic stroke.
The first high quality RCT (Michielsen et al., 2010) randomized patients to receive mirror therapy or bimanual exercise training with sight of both hands. Upper extremity spasticity was measured by the Tardieu Scale at post-treatment (6 weeks) and follow-up (6 months). There was no significant between-group difference at either time point.
The second high quality RCT (Lin et al., 2014) randomized patients to receive mirror therapy, mirror therapy + electrical stimulation, or conventional rehabilitation (task-oriented training). Upper extremity tone in the biceps, flexor carpi radialis and flexor carpi ulnaris was measured by Myoton-3 myometer at post-treatment (4 weeks). There were no significant between-group differences.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is not more effective than comparison interventions (bimanual exercises with sight of both hands, task-oriented training, mirror therapy + electrical stimulation) in reducing upper extremity spasticity/tone in patients with chronic stroke.
Upper extremity usage
Not effective
1B
One high quality RCT (Michielsen et al., 2010) investigated the effect of mirror therapy on amount of upper extremity use in patients with chronic stroke. This high quality RCT randomized patients to receive mirror therapy or bimanual exercises with sight of both hands. Upper extremity use was measured by the Stroke Upper Limb Activity Monitor at post-treatment (6 weeks). No significant between-group difference was found at either time point.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is not more effective than a comparison therapy (bimanual exercises with sight of both hands) in improving upper extremity usage in patients with chronic stroke.
Phase not specific to one period
One fair quality RCT (Amasyali & Yaliman, 2016) investigated the effect of mirror therapy on dexterity in patients with stroke. This fair quality RCT randomized patients with subacute / chronic stroke to receive mirror therapy, electrostimulation or no additional treatment; all participants received conventional rehabilitation. Dexterity was measured by the Box and Block Test at post-treatment (3 weeks) and follow-up (3 months). Significant between-group differences were found at follow-up only, in favour of mirror therapy vs. electrostimulation and no additional treatment.
Note: There was no significant difference between electrostimulation and no additional treatment.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is not more effective than comparison interventions (electrostimulation, no additional treatment) for improving dexterity in patients with stroke.
Note: However, significant between-group differences were found at follow up, in favour of mirror therapy vs. electrostimulation and no additional treatment.
Functional independence
Conflicting
4
Two high quality RCTs (Yavuzer et al., 2008; Purvane Vural et al., 2016) investigated the effect of mirror therapy on functional independence in patients with stroke.
The first high quality RCT (Yavuzer et al., 2008) randomized patients with subacute / chronic stroke to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Functional independence was measured by the Functional Independence Measure (FIM – Self-care score) at post-treatment (4 weeks) and follow-up (6 months). A significant between-group difference was found at both time points, in favour of mirror therapy vs. sham mirror therapy.
The second high quality RCT (Purvane Vural et al., 2016) randomized patients with subacute/chronic stroke to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Functional independence was measured by the FIM – Motor score at post-treatment (4 weeks). No significant between-group difference was found.
Conclusion: There is conflicting evidence (Level 4) regarding the effect of mirror therapy on functional independence following stroke. While one high quality RCT found that mirror therapy was more effective than sham mirror therapy, a second high quality RCT reported no significant difference between mirror therapy vs. no mirror therapy.
Note: The two studies used different measures of functional independence (FIM Self Care items vs. FIM Motor score), which may account for discrepancies in results.
Grip strength
Not effective
2A
One fair quality RCT (Amasyali & Yaliman, 2016) investigated the effect of mirror therapy on grip strength in patients with stroke. This fair quality RCT randomized patients with subacute / chronic stroke to receive mirror therapy, electrostimulation or no additional treatment; all participants received conventional rehabilitation. Grip strength was measured by handheld dynamometer at post-treatment (3 weeks) and follow-up (3 months). No significant between-group differences were found at either time point.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is not more effective than a comparison intervention (electrostimulation) or no treatment for improving grip strength in patients with stroke.
Motor function
Effective
1B
One high quality RCT (Purvane Vural et al., 2016), one fair quality RCT (Amasyali & Yaliman, 2016) and one poor quality RCT (Rajappan et al., 2015) investigated the effect of mirror therapy on upper extremity motor function in patients with stroke.
The high quality RCT (Purvane Vural et al., 2016) randomized patients with subacute / chronic stroke to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor function was measured by the Fugl-Meyer Assessment – Upper Extremity (FMA-UE – Wrist, Hand scores) at post-treatment (4 weeks). Significant between-group differences were found on both scores, in favour of mirror therapy vs. no mirror therapy.
The fair quality RCT (Amasyali & Yaliman, 2016) randomized patients with subacute / chronic stroke to receive mirror therapy, electrostimulation or no additional treatment; all participants received conventional rehabilitation. Upper extremity motor function was measured by the FMA-UE at post-treatment (3 weeks) and follow-up (3 months). A significant between-group difference was found at post-treatment only, in favour of mirror therapy vs. no additional treatment.
Note: There were no significant differences between mirror therapy vs. electrostimulation, or between electrostimulation vs. no additional treatment at either time point.
The poor quality RCT (Rajappan et al., 2015) randomized patients with subacute / chronic stroke to receive mirror therapy or sham mirror therapy; all participants received conventional rehabilitation. Upper extremity motor function was measured by the FMA-UE (Total, Wrist, Hand, Speed scores) and the Upper Extremity Functional Index at post-treatment (4 weeks). Significant between-group differences were found on all scores, in favour of mirror therapy vs. sham mirror therapy.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT, one fair quality RCT and one poor quality RCT that mirror therapy is more effective than comparison interventions (no mirror therapy, sham mirror therapy) for improving upper extremity motor function in patients with stroke.
Motor recovery
Conflicting
4
Two high quality RCTs (Yavuzer et al., 2008; Purvane Vural et al., 2016) investigated the effect of mirror therapy on upper extremity motor recovery in patients with stroke.
The first high quality RCT (Yavuzer et al., 2008) randomized patients with subacute / chronic stroke to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity motor recovery was measured by the Brunnstrom stages of motor recovery (Upper extremity, Hand change scores) at post-treatment (4 weeks) and follow-up (6 months). Significant between-group differences were found at both time points, in favour of mirror therapy vs. sham mirror therapy.
The second high quality RCT (Purvane Vural et al., 2016) randomized patients with subacute/chronic stroke to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity motor recovery was measured by the Brunnstrom stages of motor recovery (Upper Extremity, Hand scores) at post-treatment (4 weeks). No significant between-group differences were found.
Conclusion: There is conflicting evidence (Level 4) regarding the effect of mirror therapy on upper extremity motor recovery following stroke. While one high quality RCT found that mirror therapy was more effective than sham mirror therapy, a second high quality RCT reported no significant difference between mirror therapy vs. no mirror therapy.
One high quality RCT (Purvane Vural et al., 2016) investigated the effect of mirror therapy on pain in patients with stroke. This high quality RCT randomized patients with subacute / chronic stroke to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Pain was measured by a visual analogue scale at post-treatment (4 weeks). A significant between-group difference was found, in favour of mirror therapy vs. no mirror therapy.
Conclusion: There is moderate evidence (Level 1b) from one high quality RCT that mirror therapy is more effective than no mirror therapy for reducing pain in patients with stroke.
Range of motion
Not effective
2A
One fair quality RCT (Amasyali & Yaliman, 2016) investigated the effect of mirror therapy on range of motion in patients with stroke. This fair quality RCT randomized patients with subacute/chronic stroke to receive mirror therapy, electrostimulation or no additional treatment; all participants received conventional rehabilitation. Wrist range of motion was measured by goniometer at post-treatment (3 weeks) and follow-up (3 months). A significant between-group difference was found at follow-up only, in favour of mirror therapy vs. no additional treatment.
Note: A significant between-group difference was found at follow-up in favour of electrostimulation vs. no additional therapy.
Conclusion: There is limited evidence (Level 2a) from one fair quality RCT that mirror therapy is not more effective than a comparison intervention (electrostimulation) or no additional treatment for improving range of motion (wrist) in patients with stroke.
Spasticity
Not effective
1A
Two high quality RCTs (Yavuzer et al., 2008; Purvane Vural et al., 2016) investigated the effect of mirror therapy on upper extremity spasticity in patients with stroke.
The first high quality RCT (Yavuzer et al., 2008) randomized patients with subacute / chronic stroke to receive mirror therapy or sham mirror therapy; both groups received conventional rehabilitation. Upper extremity spasticity was measured by the Modified Ashworth Scale (MAS) at post-treatment (4 weeks) and follow-up (6 months). No significant between-group difference was found at either time point.
The second high quality RCT (Purvane Vural et al., 2016) randomized patients with subacute / chronic stroke to receive mirror therapy or no mirror therapy; both groups received conventional rehabilitation. Upper extremity spasticity was measured by the MAS at post-treatment (4 weeks). No significant between-group difference was found.
Conclusion: There is strong evidence (Level 1a) from two high quality RCTs that mirror therapy is not more effective than a comparison intervention (sham mirror therapy) or no mirror therapy for reducing upper extrremity spasticity in patients with stroke.
Clinician How-To
Pocket card
Pocket_Card_mirror_therapy
What is mirror therapy?
In mirror therapy, a mirror is placed in the client’s sagittal plane so the client cannot see the affected upper limb. The client watches in the mirror the movements made with the healthy limb and simultaneously tries to move the affected limb on the other side of the mirror. To explain why the reflection of the healthy limb in the mirror helps with the motor recovery of the affected limb, the current hypothesis is that the mirror neurons in the brain are activated during the imitation movements and interact simultaneously with the motor neurons.
Who should have mirror therapy?
Regarding the affective dimension , one of the main elements to consider is the client’s motivation to commit to the treatment process since it requires an almost daily investment of time. Mirror therapy is not recommended for clients who have a recent history of alcohol or drug abuse, severe depression or claustrophobia because these elements could interfere with the treatment.
Regarding the cognitive dimension , the key element is that the client must be able to follow instructions. Clients with cognitive disorders, aphasia, dementia, a mental health problem or attention deficit could have the therapy as long as these problems do not interfere with their understanding of the instructions and thus with the treatment for 30 minutes each day.
It is even more important to consider cognitive difficulties for clients who wish to have the therapy at home since they must be able to participate in self-directed treatment. This means they must not only be able to administer the therapy themselves, they must also be able to manage the treatment schedule, manage the material and how it is set up, keep their attention on the mirror without being reminded, self-correct, etc.
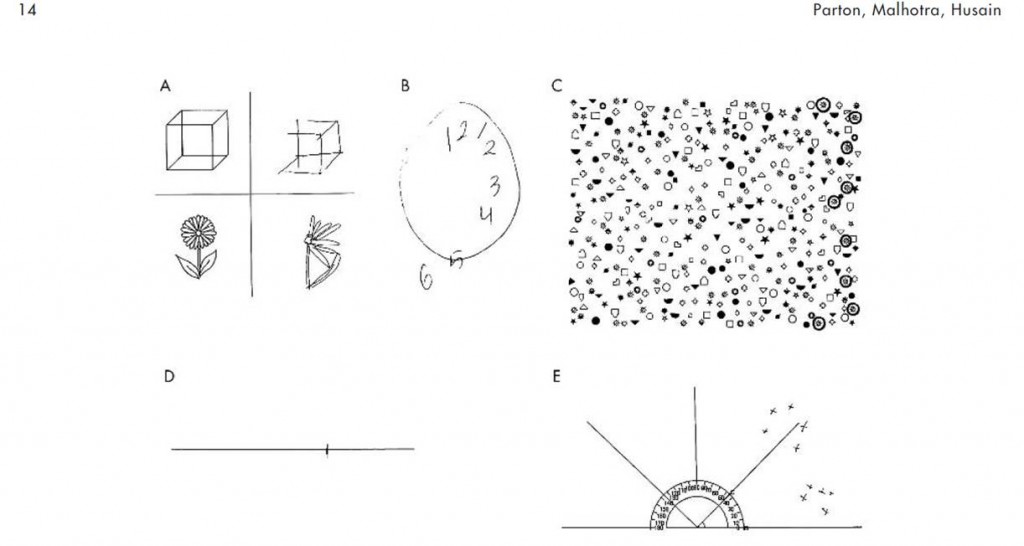
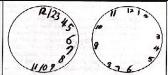
Clients with hemispatial neglect can have mirror therapy. Some studies exclude them from their research protocol but this is because their research objectives focus more specifically on the motor or functional recovery of the affected upper limb. Hemispatial neglect is excluded from their sample so that it cannot interfere with the expected results. Furthermore, clients who present severe hemispatial neglect and cannot turn their head on the contralateral side of the lesion upon request cannot have the therapy since they would not be able to keep their attention on the mirror.
Regarding the physical dimension , studies include both men and women, right- or left-handed, regardless of whether the affected side is the dominant side or not. The stroke may be ischemic or hemorrhagic with a cortical or subcortical lesion. Clients may present mild to severe hemiparesis as well as sensory deficits (paresthesia). They must be medically stable and able to maintain a sitting position throughout the treatment. Clients with vision impairments, apraxia and neurological disorders are usually excluded from studies for research purposes. Therefore, it is not known if mirror therapy is effective in the presence of these problems.
Who can give the therapy?
Mirror therapy is often given by occupational therapists and physiotherapists but any health professional can administer it.
It can also be given by a family caregiver or be self-administered following a brief explanation of how to do it and after receiving tools to do the therapy at home (user guide, written explanations, photos or videos of the movements to be done). It is important to do a regular follow-up (once a week) with clients doing the therapy at home, with or without the help of a family caregiver. The aim is to verify that the client is following instructions, understands the exercises and applies them correctly, is not making any compensating movements or taking the wrong position. The aim is also to vary the degree of difficulty, answer the client’s questions, etc. The follow-up can be done on the phone, at personal meetings, in a journal, etc. If the mirror therapy is done at home, it is important to consider the motivation of carers and the client to commit to the treatment.
If the hemiparesis is too severe and the client cannot reproduce with the affected side, simultaneously and as accurately as possible, the movements made with the healthy side, a therapist may be needed to guide or control the movements on the affected side passively. Hence it would be more difficult for such clients to do the therapy at home.
How is mirror therapy administered?
The person who administers the mirror therapy can stand in front of the client on the other side of the table. This person supervises the movements made on each side of the mirror and ensures that the client is really looking at the reflection of his/her healthy limb in the mirror.
How many weeks should mirror therapy last?
Between 3 and 6 weeks but most studies have a 4-week protocol.
How many times per week?
A minimum of 5 days per week.
How long does a mirror therapy session last?
A minimum of 30 minutes per day. This can be split into two shorter periods during the day.
What can be done in front of the mirror?
What voluntary movements are done in front of the mirror?
- Flexion and extension of the shoulder
- Flexion and extension of the elbow
- Flexion and extension of the wrist
- Flexion and extension of the fingers
- Abduction and adduction of the shoulder
- Abduction and adduction of the fingers
- Internal and external rotation of the shoulder
- Pronation and supination of the forearm
- Ulnar and radial deviation of the wrist
- Circumduction of the wrist
What actions can be done in front of the mirror?
Some examples of actions:
- Squeeze and release the fist
- Open and close the hand
- Tap the fingers on the table
- Oppose (touch) each finger to the thumb one by one
- With the hand closed, try to lift each finger, including the thumb, one at a time
What tasks can be done in front of the mirror?
Some examples of tasks:
- Handle objects using different types of grips, for example, make small balls of theraplast or modeling clay with the fingers, turn a cylindrical object in the hand (complex rotation), pick up beads or paper clips, put clothes pegs on the lip of a mug, insert pegs in a board, etc.
- Grasp and release objects with different textures (balls, sponges, etc.)
- Pick up and move various objects (balls, sticks, cubes, mug, glass, etc.) in different directions, for example, move an object following a sequence of movements forming a square or an ‘X’, put a ball in a glass and take it out, lift a glass, lift a rectangular object, place beads or pegs in a container with a small opening, insert pegs in holes in a piece of wood, transfer grains of rice from one pot to another, manipulate rings, etc.
- Turn over playing cards
- Color, connect the dots to make a drawing, copy shapes on a piece of paper
- Use different shaped stamps with an ink pad
- Handle utensils
- Wipe, clean and dust the table with cloths with different textures (scouring pad, soft sponge, silk cloth, etc.)
How must the movements be done?
The movements in front of the mirror must be done simultaneouly on the affected and the non-affected side. This encourages bilateral use of the upper limbs. If the mirror therapy involves use of an object by the healthy upper limb, the affected upper limb must try to reproduce the movement as accurately as possible but without the object.
At what speed must the movements be done?
- The client can choose the speed of the movements.
- Some studies combining the mirror with electrical stimuli suggest that the voluntary movements are done in 5 or 10 seconds. The time the movements take must match the duration of the electrical stimuli.
What assistance is offered during the sessions?
- The emphasis should be on active movements in front of the mirror. Clients must try their best to make the same movements with their affected upper limb. According to some studies, assistance can be offered to make the movements with the affected upper limb passively, especially if the hemiparesis is severe. To date, there is no consensus regarding whether physical assistance interferes with the mirror therapy treatment.
- The desired movement may be demonstrated.
- The client can be given an instruction booklet containing written instructions, photos or videos of the movements, actions and tasks to be done, especially if the mirror therapy is done at home. A toolbox containing the material needed to use the mirror may also be offered or loaned to the client.
- The client can use a journal, especially if the therapy is done at home, as a tool to help with follow-up and to inform the therapists of the progress of the therapy (mirror therapy schedule, client’s experiences, exercises done, etc.).
What assessments and other intervention can be done with mirror therapy?
Studies exploring mirror therapy have used different assessments to measure participants’ progress, including:
- Fugl-Meyer Assessment to measure motor recovery of the upper limb
- Brunnstrom Scale to measure the type of movement done
- Demeurisse Motricity Index for the upper limb to assess motor function
- Action Research Arm Test (ARAT) to measure specific changes in upper limb activity
- Functional Independence Measure (FIM)
There are no contraindications to using mirror therapy at the same time as other therapies. In fact, some studies combine training on specific tasks, bilateral use of the upper limbs and electrical stimuli with the use of mirror therapy.
What are the side effects of mirror therapy?
Study participants have not reported any side effects. However, one study reported that some participants got bored during the therapy.
What important features must the mirror have?
- The mirror is placed in the client’s midsagittal plane. The client must watch the reflection of his/her healthy limb in the mirror in order to simulate that the image is actually of the affected upper limb.
- Different materials can be used to build the structure of the mirror (wood, corrugated cardboard, plastic, etc.).
- The size of the mirror can vary between 12 in x 12 in and 28 in x 48 in. Its size depends on the types of movements to be done in front of the mirror.
- To ensure that the client cannot see it behind the mirror, the affected upper limb can be inserted in an enclosed box or the affected hand can be covered by a screen.
- One study designed a folding mirror that is easy to carry. The angle of the mirror is supported by velcro strips.
What else is important to remember before using the mirror?
All jewelry and watches must be removed so that the illusion of the reflection is as credible as possible.
When and in what settings can mirror therapy be used?
When is the best time to have mirror therapy?
Mirror therapy has positive results in the acute, subacute and chronic phase post-stroke. Most studies advocate early intervention (as soon as possible) up to 14 months post-stroke.
In what settings can mirror therapy be used?
Mirror therapy can be used in different settings, including in the hospital (acute care), in-patient rehabilitation, out-patient rehabilitation and at home. The treatment setting varies with the client’s level of functional and socio-residential autonomy.
Mirror therapy can be done at home, self-administered or supervised by a family caregiver. However, clinical reasoning must be used before determining if a client is eligible.
Can mirror therapy be given in a group?
Mirror therapy can be given individually or in a group. However, including clients with attention deficits or hemispatial neglect in a group is not recommended because there is less progress in a group with respect to reducing hemispatial neglect.
References used in this section
Altschuler, E. L., et al. (1999). “Rehabilitation of hemiparesis after stroke with a mirror.” The Lancet 353(9169): 2035-2036.
Arya, K. N. and S. Pandian (2013). “Effect of task-based mirror therapy on motor recovery of the upper extremity in chronic stroke patients: a pilot study.” Topics in Stroke Rehabilitation 20(3): 210-217.
Cacchio, A., et al. (2009). “Mirror therapy for chronic complex regional pain syndrome type 1 and stroke.” New England Journal of Medicine 361(6): 634-636.
Cacchio, A., et al. (2009). “Mirror therapy in complex regional pain syndrome type 1 of the upper limb in stroke patients.” Neurorehabilitation & Neural Repair 23(8): 792-799.
de Almeida Oliveira, R., et al. (2014). “Mental practice and mirror therapy associated with conventional physical therapy training on the hemiparetic upper limb in poststroke rehabilitation: a preliminary study.” Topics in Stroke Rehabilitation 21(6): 484-494.
Dohle, C., et al. (2009). “Mirror therapy promotes recovery from severe hemiparesis: a randomized controlled trial.” Neurorehabilitation & Neural Repair 23(3): 209-217.
Ezendam, D., et al. (2009). “Systematic review of the effectiveness of mirror therapy in upper extremity function.” Disability & Rehabilitation 31(26): 2135-2149.
Faralli, A., et al. (2013). “Noninvasive strategies to promote functional recovery after stroke.” Neural Plasticity 2013: 854597.
Invernizzi, M., et al. (2013). “The value of adding mirror therapy for upper limb motor recovery of subacute stroke patients: a randomized controlled trial.” European journal of physical & rehabilitation medicine. 49(3): 311-317.
Kim, H., et al. (2014). “Effect of functional electrical stimulation with mirror therapy on upper extremity motor function in poststroke patients.” Journal of Stroke & Cerebrovascular Diseases 23(4): 655-661.
Kojima, K., et al. (2014). “Feasibility study of a combined treatment of electromyography-triggered neuromuscular stimulation and mirror therapy in stroke patients: a randomized crossover trial.” Neurorehabilitation 34(2): 235-244.
Lee, M. M., et al. (2012). “The mirror therapy program enhances upper-limb motor recovery and motor function in acute stroke patients.” American Journal of Physical Medicine & Rehabilitation 91(8): 689-696, quiz 697-700.
Lin, K. C., et al. (2014). “Combining afferent stimulation and mirror therapy for rehabilitating motor function, motor control, ambulation, and daily functions after stroke.” Neurorehabilitation & Neural Repair 28(2): 153-162.
Lisa, L. P., et al. (2013). “The effectiveness of different treatment modalities for the rehabilitation of unilateral neglect in stroke patients: a systematic review.” Neurorehabilitation 33(4): 611-620.
Michielsen, M. E., et al. (2011). “Motor recovery and cortical reorganization after mirror therapy in chronic stroke patients: a phase II randomized controlled trial.” Neurorehabilitation & Neural Repair 25(3): 223-233.
Nilsen, D. M. and T. DiRusso (2014). “Using mirror therapy in the home environment: a case report.” American Journal of Occupational Therapy 68(3): e84-89.
Pandian, J. D., et al. (2014). “Mirror therapy in unilateral neglect after stroke (MUST trial): a randomized controlled trial.” Neurology 83(11): 1012-1017.
Pollock, A., et al. (2014). “Interventions for improving upper limb function after stroke.” Cochrane Database of Systematic Reviews 11: CD010820.
Radajewska, A., et al. (2013). “The effects of mirror therapy on arm and hand function in subacute stroke in patients.” International Journal of Rehabilitation Research 36(3): 268-274.
Rothgangel, A. S., et al. (2011). “The clinical aspects of mirror therapy in rehabilitation: a systematic review of the literature.” International Journal of Rehabilitation Research 34(1): 1-13.
Samuelkamaleshkumar, S., et al. (2014). “Mirror therapy enhances motor performance in the paretic upper limb after stroke: a pilot randomized controlled trial.” Archives of Physical Medicine & Rehabilitation 95(11): 2000-2005.
Sathian, K., et al. (2000). “Doing it with mirrors: a case study of a novel approach to neurorehabilitation.” Neurorehabilitation & Neural Repair 14(1): 73-76.
Shinoura, N., et al. (2008). “Mirror therapy activates outside of cerebellum and ipsilateral M1.” Neurorehabilitation 23(3): 245-252.
Stevens, J. A. and M. E. P. Stoykov (2003). “Using motor imagery in the rehabilitation of hemiparesis.” Archives of physical medicine and rehabilitation 84(7): 1090-1092.
Thieme, H., et al. (2012). “Mirror therapy for improving motor function after stroke.” Cochrane Database of Systematic Reviews 3: CD008449.
Thieme, H., et al. (2013). “Mirror therapy for patients with severe arm paresis after stroke–a randomized controlled trial.” Clinical Rehabilitation 27(4): 314-324.
Wang, J., et al. (2013). “Cerebral activation evoked by the mirror illusion of the hand in stroke patients compared to normal subjects.” Neurorehabilitation 33(4): 593-603.
Wu, C. Y., et al. (2013). “Effects of mirror therapy on motor and sensory recovery in chronic stroke: a randomized controlled trial.” Archives of Physical Medicine & Rehabilitation 94(6): 1023-1030.
Yavuzer, G., et al. (2008). “Mirror therapy improves hand function in subacute stroke: a randomized controlled trial.” Archives of Physical Medicine & Rehabilitation 89(3): 393-398.
Yun, G. J., et al. (2011). “The synergic effects of mirror therapy and neuromuscular electrical stimulation for hand function in stroke patients.” Annals of Rehabilitation Medicine 35(3): 316-321.
Info Pocket Booklet
Pocket Card for mirror therapy
References
Altschuler, E.L., Wisdom, S.B., Stone, L., Foster, C., Galasko, D., Llewellyn, M.E., & Ramachandran, V.S. (1999). Rehabilitation of hemiparesis after stroke with a mirror. The Lancet, 353, 2035-2036. doi: 10.1016/S0140-6736(99)00920-4
Amasyali, S.Y. & Yaliman, A. (2016). Comparison of the effects of mirror therapy and electromyography-triggered neuromuscular stimulation on hand functions in stroke patients: a pilot study. International Journal of Rehabilitation Research, 39, 302-7. doi: 10.1097/MRR.0000000000000186
Arya, K.N., Pandian, S., Kumar, D., & Puri, V. (2015). Task-based mirror therapy augmenting motor recovery in poststroke hemiparesis: a randomized controlled trial. Journal of Stroke & Cerebrovascular Diseases, 24(8), 1738-48. doi: 10.1016/j.jstrokecerebrovasdis.2015.03.026
Bae, S.H., Jeong, W.S., & Kim, K.Y. (2012). Effects of mirror therapy on subacute stroke patients’ brain waves and upper extremity functions. Journal of Physical Therapy Science, 24(11), 1119-22. doi: 10.1589/jpts.24.1119
Cacchio, A., De Blasis, E., De Blasis, V., Santilli, V., & Spacca, G. (2009a). Mirror therapy in Complex Regional Pain Syndrome type 1 of the upper limb in stroke patients. Neurorehabilitation and Neural Repair, 23, 792-799. doi: 10.1177/1545968309335977
Cacchio, A., De Blasis, E., Necozione, S., di Orio, F., & Santilli, V. (2009b). Mirror therapy for Chronic Complex Regional Pain Syndrome type 1 and stroke. New England Journal of Medicine, 361(6), 634-636. doi: 10.1056/NEJMc0902799
Cho, H.-S. & Cha, H.-G. (2015). Effect of mirror therapy with tDCS on functional recovery of the upper extremity of stroke patients. Journal of Physical Therapy Science, 27, 1045-7. doi: 10.1589/jpts.27.1045
Colomer, C., Noe, E., & Llorens, R. (2016). Mirror therapy in chronic stroke survivors with severely impaired upper limb function: a randomized controlled trial. European Journal of Physical and Rehabilitation Medicine, 52(3), 271-8. Retrieved from: http://www.minervamedica.it/en/journals/europa-medicophysica/article.php?cod=R33Y2016N03A0271
Costa, V.S, Silveira, J.C.C., Clementino, T.C.A., Borges, L.R.D.M., & Melo, L.P. (2016). Effects of mirror therapy on the motor and functional recovery of post-stroke paretic upper limbs: a systematic review. Fisioterapia e Pesquisa, 23(4), 431-8. doi: 10.1590/1809-2950/15809523042016
Dohle, C., Püllen, J., Nakaten, A., Küst, J., Rietz, C., & Karbe, H. (2009). Mirror therapy promotes recovery from severe hemiparesis: a randomized controlled trial. Neurorehabilitation and Neural Repair, 23, 209-217. doi: 10.1177/1545968308324786
Ezendam, D., Bongers, R. M., Jannink, M. J. A. (2009). Systematic review of the effectiveness of mirror therapy in upper extremity function. Disability and Rehabilitation, 31, 2135-2149. doi: 10.3109/09638280902887768
Gurbuz, N., Afsar, S.I., Ayas, S., & Cosar, S.N.S. (2016). Effect of mirror therapy on upper extremity motor function in stroke patients: a randomized controlled trial. The Journal of Physical Therapy Science, 28(9), 2501-6. DOI: 10.1589/jpts.28.2501
Invernizzi, M., Negrini, S., Cara, S., Lanzotti, L., Cisari, C., & Baricich, A. (2013). The value of adding mirror therapy for upper limb motor recovery of subacute stroke patients: a randomized controlled trial. European Journal of Physical and Rehabilitation Medicine, 49(3), 311-7. Retrieved from: https://www.minervamedica.it/en/journals/europa-medicophysica/article.php?cod=R33Y2013N03A0311
Ji, S.-G., Cha, H.-G., & Kim, M.-K. (2014). Stroke recovery can be enhanced by using repetitive transcranial magnetic stimulation combined with mirror therapy. Journal of Magnetics, 19(1), 28-31. doi: 10.4283/JMAG.2014.19.1.028
Kim, K., Lee, S., Kim, D., Lee, K., & Kim, Y. (2016). Effects of mirror therapy combined with motor tasks on upper extremity function and activities daily living of stroke patients. Journal of Physical Therapy Science, 28(2), 483-7. doi: 10.1589/jpts.28.483
Kim, H.J., Lee, G.C., & Song, C.H. (2014). Effect of functional electrical stimulation with mirror therapy on upper extremity motor function in poststroke patients. Journal of Stroke and Cerebrovascular Diseases, 23(4), 655-61. doi: 10.1016/j.jstrokecerebrovasdis.2013.06.017
Lee, M.M., Cho, H., & Song, C.H. (2012). The mirror therapy program enhances upper-limb motor recovery and motor function in acute stroke patients. American Journal of Physical Medicine & Rehabilitation, 91(8), 689-700. doi: 10.1097/PHM.0b013e31824fa86d
Lim, K.-B., Lee, H.-J., Yoo, J., Yun, H.-J., & Hwang, H.-J. (2016). Efficacy of mirror therapy containing functional tasks in poststroke patients. Annals of Rehabilitation Medicine, 40(4), 629-36. doi: 10.5535/arm.2016.40.4.629
Lin, K.-C., Huang, P.-C., Chen, Y.-T., Wu, C.-Y., & Huang, W.-L. (2014). Combining afferent stimulation and mirror therapy for rehabilitating motor function, motor control, ambulation, and daily functions after stroke. Neurorehabilitation and Neural Repair, 28(2), 153-62. doi: 10.1177/1545968313508468
Michielsen, M. E., Selles, R. W., van der Geest, J. N., Eckhardt, M., Yavuzer, G., Stam, H. J., Smits, M., Ribbers, G. M., & Bussmann, J. B. J. (2010). Motor recovery and cortical reorganization after mirror therapy in chronic stroke patients: a phase II randomized controlled trial. Neurorehabilitaiton and Neural Repair, 4, 1-11. doi: 10.1177/1545968310385127
Mirela, C.L., Matei, D., Ignat, B., & Popescu, C.D. (2015). Mirror therapy enhances upper extremity motor recovery in stroke patients. Acta Neurologica Belgica, 115, 597-603. doi: 10.1007/s13760-015-0465-5
Nagapattinam, S., Vinod Babu, K., Sai Kumar, N., & Ayyappan, V.R. (2015). Effect of task specific mirror therapy with functional electrical stimulation on upper limb function for subacute hemiplegia. International Journal of Physiotherapy, 2(5), 840-9. doi: 10.15621/ijphy/2015/v2i5/78243
Pandian, J.D., Arora, R., Kaur, P., Sharma, D., Vishwambaran, D.K., & Arima, H. (2014). Mirror therapy in unilateral neglect after stroke (MUST trial): a randomized controlled trial. Neurology, 83, 1012-7. doi: 10.1212/WNL.0000000000000773
Park, J.-Y., Chang, M., Kim, K.-M., & Kim, H.J. (2015a). The effect of mirror therapy on upper-extremity function and activities of daily living in stroke patients. Journal of Physical Therapy Science, 27, 1681-3. doi: 10.1589/jpts.27.1681
Park, Y., Chang, M., Kim, K.-M., & An, D.-H. (2015b). The effects of mirror therapy with tasks on upper extremity function and self-care in stroke patients. Journal of Physical Therapy Science, 27, 1499-501. doi: 10.1589/jpts.27.1499
Purvane Vural, S., Yuzer, G.F.N., Ozcan, D.S., Ozbudak, S.D., & Ozgirgin, N. (2016). Effects of mirror therapy in stroke patients with complex regional pain syndrome type 1: a randomized controlled study. Archives of Physical Medicine and Rehabilitation, 97, 575-81. doi: 10.1016/j.apmr.2015.12.008
Radajewska, A., Opara, J.A., Kucio, C., Blaszczyszyn, M., Mehlich, K., Szczygiel, J. (2013). The effects of mirror therapy on arm and hand function in subacute stroke in patients. International Journal of Rehabilitation Research, 36(3), 268-74. doi: 10.1097/MRR.0b013e3283606218
Radajewska, A., Opara, J., Bilinski, G., Kaczorowska, A., Nawrat-Szoltysik, A., Kucinsak, A., &. Lepsy, E. (2017). Effectiveness of mirror therapy for subacute stroke in relation to chosen factors. Rehabilitation Nursing, 42(4), 223-9. doi: 10.1002/rnj.275
Rajappan, R., Abudaheer, S., Selvaganapathy, K., & Gokanadason, D. (2015). Effect of mirror therapy on hemiparetic upper extremity in subacute stroke patients. International Journal of Physiotherapy, 2(6), 1041-6. doi: 10.15621/ijphy/2015/v2i6/80766
Rehani, P., Kumari, R., & Midha, D. (2015). Effectiveness of motor relearning programme and mirror therapy on hand functions in patients with stroke – a randomized clinical trial. International Journal of Therapies and Rehabilitation Research, 4(3), 20-4. doi: 10.5455/ijtrr.00000058
Rodrigues, L.C., Farias, N.C., Gomes, R.P., & Michaelsen, S.M. (2016). Feasibility and effectiveness of adding object-related bilateral symmetrical training to mirror therapy in chronic stroke: a randomized controlled pilot study. Physiotherapy Theory and Practice, 32(2), 83-91. doi: 10.3109/09593985.2015.1091872
Rothgangel, A. S., Braun, S. M., Beurskens, A. J., Seitz, R. J., & Wade, D. T. (2011). The clinical aspects of mirror therapy in rehabilitation: A systematic review of the literature. International Journal of Rehabilitation Research, 34, 1-13. doi: 10.1097/MRR.0b013e3283441e98
Samuelkamaleshkumar, S., Reethajanetsureka, S., Pauljebaraj, P., Benshamir, B., Padankatti, S.M., David, J.A. (2014). Mirror therapy enhances motor performance in the paretic upper limb after stroke: a pilot randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 95(11), 2000-5. doi: 10.1016/j.apmr.2014.06.020
Thieme, H., Bayn, M., Wurg, M., Zange, C., Pohl, M., & Behrens, J. (2012). Mirror therapy for patients with severe arm paresis after stroke – a randomized controlled trial. Clinical Rehabilitation, 27(4), 314-24. doi: 10.1177/0269215512455651
Wu, C.-Y., Huang, P.-C., Chen, Y.-T., Lin, K.-C., & Yang, H.-W. (2013). Effects of mirror therapy on motor and sensory recovery in chronic stroke: a randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 94, 1023-30. doi: 10.1016/j.apmr.2013.02.007
Yavuzer G., Selles R., Sezer N., Sütbeyaz S., Bussmann J.B., Köseoglu F., Atay M.B., Stam H.J.(2008). Mirror Therapy Improves Hand Function in Subacute Stroke: A Randomized Controlled Trial. Archive of Physical Medicine, 89, 393-398. doi: 10.1016/j.apmr.2007.08.162
Yeldan, I., Huseyinsinoglu, B.E., Akinci, B., Tarakci, E., Baybas, S., & Ozdincler, A.R. (2015). The effects of very early mirror therapy on functional improvement of the upper extremity in acute stroke patients. Journal of Physical Therapy Science, 27, 3519-24. doi: 10.1589/jpts.27.3519
Yun, G.J., Chun, M.H., Park, J.Y., & Kim, B.R. (2011). The synergic effects of mirror therapy and neuromuscular electrical stimulation for hand function in stroke patients. Annals of Rehabilitation Medicine, 35, 316-21. doi: 10.5535/arm.2011.35.3.316
Excluded Studies
Arya, K.N. & Pandian, S. (2013). Effect of task-based mirror therapy on motor recovery of the upper extremity in chronic stroke patients: a pilot study. Topics in Stroke Rehabilitation, 20(3), 210-7. doi: 10.1310/tsr2003-210
Reason for exclusion: Not a randomized controlled trial.
Dalla Libera, D., Regazzi, S., Fasoletti, C., Dinacci Ruggieri, D., & Rossi Hildebrand, P. (2015). Beneficial effect of transcranial magnetic stimulation combined with mirror therapy in stroke patients: a pilot study in neurorehabilitative setting. Brain Stimulation, 8, 360-77. doi: 10.1016/j.brs.2015.01.206
Reason for exclusion: Abstract only – statistical data of clinical outcome measures not provided.
Geller, D., Nilsen, D., Van Lew, S., Gillen, G., & Bernardo, M. (2016). Home mirror therapy: a randomized controlled pilot study comparing unimanual and bimanual mirror therapy for improved upper limb function post-stroke. Archives of Physical Medicine and Rehabilitation, 97(10), e4. doi: 10.1016/j.apmr.2016.08.008
Reason for exclusion: Oral presentation – no statistical data provided for clinical outcome measures.
Harmsen, W., Bussmann, J.B.J., Selles, R.W., Hurkmans, H.L.P., & Ribbers, G.M. (2015). A mirror therapy-based action observation protocol to improve motor learning after stroke. Neurorehabilitation and Neural Repair, 29(6), 509-16. doi: 10.1177/1545968314558598
Reason for exclusion: Observational study; intervention provided over one session.
Ju, Y. & Yoon, I.-J. (2018). The effects of modified constraint-induced movement therapy and mirror therapy on upper extremity function and its influence on activities of daily living. The Journal of Physical Therapy Science, 30, 77-81. doi: 10.1589/jpts.30.77
Reason for exclusion: No between-group comparisons.
Kim, H. & Shim, J. (2015). Investigation of the effects of mirror therapy on the upper extremity functions of stroke patients using the manual function test. The Journal of Physical Therapy Science, 27, 227-9. doi: 10.1589/jpts.27.227
Reason for exclusion: Not a randomized controlled trial; results do not add strength to current evidence.
Kojima, K., Ikuno, K., Morii, Y., Tokuhisa, K., Morimoto, S., & Shomoto, K. (2014). Feasibility study of a combined treatment of electromyography-triggered neuromuscular stimulation and mirror therapy in stroke patients: a randomized crossover trial. NeuroRehabilitation, 34, 235-44. doi: 10.3233/NRE-131038
Reason for exclusion: Combined therapy (mirror therapy + electromyography-triggered neuromuscular stimulation) impacts on ability to determine effects of mirror therapy alone.
Lee, D., Lee, G. & Jeong, J. (2016). Mirror therapy with neuromuscular electrical stimulation for improving motor function of stroke survivors: a pilot randomized clinical study. Technology and Health Care, 24(4), 503-11. doi: 10.3233/THC-161144
Reason for exclusion: Combined therapy (mirror therapy + neuromuscular electrical stimulation) impacts on ability to determine effects of mirror therapy alone.
Medeiros, C.S., Fernandes, S.G., Lopes, J.M., Cacho, E.N., & Cacho, R.O. (2014). Effects of mirror therapy through functional activities and motor standards in motor function of the upper limb after stroke. Fisioterapia & Pesquisa, 21(3), 264-70. doi: 10.590/1809-2950/87821032014.
Reason for exclusion: Both groups received mirror therapy (mirror therapy using functional activities vs. mirror therapy using isolated motor patterns).
Moustapha, A. & Rousseaux, M. (2012). Immediate effects of mirror therapy on spatial neglect. Annals of Physical and Rehabilitation Medicine, 55(S1), e197. doi: 10.1016/j.rehab.2012.07.501
Reason for exclusion: Abstract, insufficient information.
Paik, Y.-R., Kim, S.-K., Lee, J.-S., & Jeon, B.-Y. (2014). Simple and task-oriented mirror therapy for upper extremity function in stroke patients: a pilot study. Hong Kong Journal of Occupational Therapy, 24, 6-12. doi: 1016/j.hkjot.2014.01.002
Reason for exclusion: Non-randomized study with no between-group comparisons; results do not add strength to current evidence.
Rothgangel, A.S., Morton, A.R., van den Hout, J.W.E., Beurkens, A.J.H.M. (2004). Phantoms in the brain: spiegeltherapie bij chronische CVA-patienten; een pilot-study. Nederlands Tijdschrift voor Fysiotherapie, 114, 36-40. Accessed from: https://www.researchgate.net/profile/Andreas_Rothgangel/publication/290130135_Phantoms_in_the_brain_Mirror_therapy_in_chronic_stroke_patients_a_pilot_study/links/56a0b3ec08aee4d26ad74c6a/Phantoms-in-the-brain-Mirror-therapy-in-chronic-stroke-patients-a-pi
Reason for exclusion: Language other than English/French.
Selles, R.W., Michielsen, M.E., Bussmann, J.B.J., Stam, H.J., Hurkmans, H.L., Heijnen, I., Groot, D.d., Ribbers, G.M. (2014). Effects of a mirror-induced visual illusion on a reachgin task in stroke patients: implications for mirror therapy training. Neurorehabilitation and Neural Repair, 28(7), 652-9. doi: 10.1177/1545968314521005
Reason for exclusion: Not an intervention.
Salhab, G., Sarraj, A.R., & Saleh, S. (2016). Mirror therapy combined with functional electrical stimulation for rehabilitation of stroke survivors’ ankle dorsiflexion. IEEE explore digital library, 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). doi: 10.1109/EMBC.2016.7591776
Reason for exclusion: Combined therapy (mirror therapy + electrical stimulation) impacts on ability to determine effect of mirror therapy alone.
Sathian K., Greenspan A.I. & Wolf S.L. (2000). Doing It with Mirrors: A Case Study of a Novel Approach to Neurorehabilitation. Neurorehabilitation and Neural Repair, 14(1), 73-76. doi: 10.1177/154596830001400109
Reason for exclusion: Not a randomized controlled trial; results do not add to strength to current evidence.
Seok, H., Kim, S.H., Jang, Y.W., Lee, J.B., & Kim, S.W. (2010). Effect of mirror therapy on recovery of upper limb function and strength in subacute hemiplegia after stroke. Journal of Korean Academy of Rehabilitation Medicine, 34, 508-12. Accessed from: http://www.koreascience.or.kr/article/ArticleFullRecord.jsp?cn=DJHOB7_2010_v34n5_508
Reason for exclusion: Language other than English/French.
Stevens J.A., Stoykov P.M.E. (2003). Using motor imagery in the rehabilitation of hemiparesis. Archives of Physical Medicine, 84(7), 1090-2. doi: 10.1016/S0003-9993(03)00042-X
Reason for exclusion: Not a randomized controlled trial; results do not add to strength to current evidence.
Yoon, J.A., Koo, B.I., Shin, M.J., Shin, Y.B., Ko, H.-Y., & Shin, Y.-I. (2014). Effect of constraint-induced movement therapy and mirror therapy for patients with subacute stroke. Annals of Rehabilitation Medicine, 38(4), 458-66. doi: 10.5535/arm.2014.38.4.458
Reason for exclusion: Combined therapy (mirror therapy + CIMT) impacts on ability to determine effects of mirror therapy alone.
Zacharis, D., Moumtzi, E., Terzis, N., Roussos, N., & Patatoukas, D. (2014). The use of mirror therapy in stroke patients with hemiplegic upper limb: a randomized controlled trial. Annals of Physical and Rehabilitation Medicine, 57S, e27. doi: 10.1016/j.rehab.2014.03.101
Reason for exclusion: Abstract, insufficient information.