Proper positioning post-stroke is essential in order to reduce the risk of shoulder subluxation, contractures and pain. Proper positioning may also enhance motor recovery, range of motion, and oxygen saturation.
In this module we identify the evidence for optimal positioning of the patient when:
Lying: supine, on affected side and on non-affected side,
Sitting: in bed, chair and wheelchair,
Standing and transferring.
Patient/Family Information
Authors*: Erica Kader; Nicol Korner-Bitensky, PhD OT; Elissa Sitcoff, BA BSc; Leila Goulamhoussen, BSc OT; Rabiaa Laroui, BSc OT; Sheila Liu, BSc OT; Anita Petzold, BSc OT; Anna Rentoulis, BSc OT; Stephen Tang, BSc OT
What is positioning?
After a stroke, muscles can be affected in various ways, causing pain, spasticity, and problems with speed and range of motion. One way to minimize these effects is to properly support, position, and align your body. While in the hospital or rehabilitation centre, your healthcare professional will suggest ways to position your body that are safe and comfortable. This may include the teaching of proper techniques when transferring from sitting to standing, or using devices such as foam wedges or slings to maintain support.
Why is positioning important after a stroke?
Proper positioning can be useful to minimize or prevent pain and stiffness that are commonly present post-stroke. It can also help you to regain movement that was lost after your stroke, or limit future problems with movement. In addition, proper positioning has been shown to increase awareness and protection of the weaker side of the body.
Some common positions recommended following a stroke
Positioning while lying on your back: Pillows are placed behind the shoulder, head, weaker arm, and hip. The feet are placed in a neutral position.
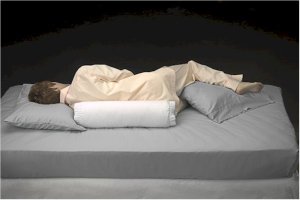
Positioning while lying on the weaker side: When lying on the weaker side, one or two pillows are placed under the head, the weaker shoulder is positioned comfortably on a pillow, the stronger leg is forward on one or two pillows, and the weaker leg is straight out. Pillows are also placed in back and in front of the body.
Positioning while lying on the stronger side: One or two pillows are placed under the head, while the weaker shoulder is placed forward with the weaker arm supported by pillows. The weaker leg is placed toward the back on pillows.
Positioning while sitting up: The individual is seated at the centre of the chair or wheelchair, their arms placed forward onto pillows on their lap or on a table. Feet are placed flat on the floor or on footrests with knees bent directly above the feet.
Positioning while sitting in bed: Sitting up in bed is recommended for short periods only as it is better to sit in a chair as soon as possible. The individual will sit upright, well supported by pillows. Arms are placed on pillows on either side of the body and legs are extended comfortably.
Positioning during transfers: During transfers to a chair or from a chair to another chair, positioning of the weaker shoulder and upper arm is important. The weaker arm should always be supported during transfers, and it is important that no one pull on the arm as it can cause pain in your shoulder that will be difficult to eliminate once created. For getting out of bed, it may be useful to install a bar beside your bed that you can hold onto with your stronger arm to help push yourself up to the standing position. Photo courtesy of www.invisiblecaregiver.com
Positioning while standing and walking: While standing up and moving around, slings and supports are used for positioning of the weaker arm.
How effective is positioning after stroke?
Preventing shoulder pain: Arm positioning while lying and sitting was shown to be ineffective in preventing shoulder pain for all stages of stroke. However positioning of the weaker arm using slings and supports while standing and moving around was shown to be effective in preventing shoulder pain. There was no evidence as to whether positioning of the shoulder and arm during transfers was effective in preventing shoulder pain but it is definitely best practice to protect the weaker arm by supporting it (and never pulling on it) during transfers.
Reducing shoulder pain: Positioning of the weaker shoulder and arm using slings and supports while standing and moving around was shown to be an effective way of reducing shoulder pain. No evidence was found to show that upper limb positioning during transfers would reduce shoulder pain. Arm positioning while lying and sitting was also found to be ineffective in reducing shoulder pain. Again it is important to note that it is definitely best practice to support the weaker arm (and never pull on it) during standing and walking.
Preventing and reducing shoulder subluxation (dislocation of the shoulder): There is conflicting scientific evidence concerning the effectiveness of arm positioning while sitting on the prevention of shoulder subluxation (dislocation). Upper limb positioning while standing and walking is effective in preventing and reducing shoulder dislocation.
Improving range of motion: Proper arm positioning while lying and sitting has been shown to be ineffective for improving arm range of motion (how much it can move through space).
Improving functional independence: Proper arm positioning while lying and sitting has been shown to be ineffective in improving ability to perform daily tasks after a stroke.
Increasing awareness of the upper limb: No evidence was found concerning the effectiveness of arm positioning while sitting to increase awareness of the weaker arm. Generally, best practice is to have the arm placed in a position where the patient is able to see the arm – for example on a lap tray if the person is sitting in a wheelchair.
What devices can I use for positioning?
Positioning devices exist for various purposes, including support and padding. Below you will find examples of some of the devices that are available to aid in positioning. Your health care provider can give you information on positioning aids that are appropriate for your specific needs.
Slings: Various slings are available and can be used following a stroke to support your weaker arm while you are standing or during transfers. Slings can prevent pain that is caused by dislocation of the shoulder.
Head Donut: This supports the back of your head when lying down.
Pillows: Pillows are used for padding and protection of some pressure points of the arm and legs, such as elbows, knees, and heels.
Wedges: Wedges are placed under your knees to prevent you from sliding in a chair while sitting down.
Lap trays: Lap trays are attached to the armrest of a wheelchair and lay across your lap. This will allow you to rest your weaker arm on the tray.
Arm trough: Arm troughs are placed on the armrest of the wheelchair to keep your weaker arm from hanging over the side. A strap can also be added to the trough to provide additional support.
Harness: These can be used for the weaker shoulder. They are often adjustable and fastened with Velcro. A shoulder harness offers support by fitting over the weaker shoulder, and passing behind the neck to strap onto the stronger arm.
Where can I get the devices to aid in positioning?
Your healthcare professional will help you to choose the devices that are appropriate for your needs as well as ensure a proper fit. If they cannot supply you with your positioning aids they will direct you to a supplier from whom you can purchase these devices. Be sure to get information from your supplier or healthcare provider on proper cleaning and maintenance of your positioning aid.
How much does it cost?
Positioning devices are available for purchase either from your rehabilitation facility, or directly from the supplying companies themselves. Suppliers range in price. It is possible that your positioning devices may be covered by your health insurance.
Are there any side effects/risks?
There are generally no side effects to proper positioning after a stroke. It is important to consult with a healthcare professional who can give you appropriate advice, since incorrect positioning can put strain on your muscles, cause discomfort, and of course will not give beneficial results.
Who can help me with positioning?
It is important that a trained healthcare professional show you how to properly and safely position your body and upper limb following a stroke. This type of advice is usually provided by a physical or occupational therapist. Your therapist can also teach proper positioning techniques to your family and friends so that they can help you as well.
Clinician Information
Note: When reviewing the findings, it is important to note that they are always made according to randomized clinical trial (RCT) criteria – specifically as compared to a control group. To clarify, if a treatment is “effective” it implies that it is more effective than the control treatment to which it was compared. Non-randomized studies are no longer included when there is sufficient research to indicate strong evidence (level 1a) for an outcome.
Positioning of the upper extremity is used to prevent pain, contractures, and shoulder subluxation and to improve motor recovery, range of motion, and oxygen saturation. We conducted a systematic review of the scientific literature to compile current knowledge regarding the effectiveness of post-stroke positioning.
The results of 17 studies including four high quality RCTs, one quasi experimental study, one case-control study, six repeated-measures studies, and five surveys were compiled to summarize the current knowledge on positioning of patients post-stroke. In addition, references from one review article were retrieved and reviewed to identify any that were research based: all were expert opinion or textbook references rather than study based.
Static arm positioning (without strapping) while lying or sitting – Acute phase
Function
Not Effective
1B
One high quality RCT (Ada et al., 2005) examined the effect of positioning the affected shoulder in lying and in sitting for improving function in 31 patients with acute stroke. Both the intervention group (n=15) and the control group (n=16) received upper extremity exercises approximately 5 x 10-minute sessions per week for 4 weeks while also receiving standard upper limb care (including slings and supports). In addition, the treatment group received static positioning of the affected arm in two different positions a day (1 lying, 1 sitting), each for 30 minutes per day, 5 days per week, for 4 weeks. The lying static position consisted of lying supine with the arm in comfortable full external rotation and 45° of abduction with elbow flexion. The sitting position consisted of sitting at a table, with both the shoulder and elbow in 90° flexion. No between-group difference was found for functional status as measured by Item 6 of the Motor Assessment Scale (MAS).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static shoulder positioning of the hemiplegic arm during supine lying and sitting does not improve function in patients witch acute stroke.
Shoulder external rotation contracture
Effective
1B
One high quality RCT (Ada et al., 2005) examined the effect of positioning the affected shoulder in lying and in sitting for the prevention of shoulder contracture in 31 patients with acute stroke. Both the intervention group (n=15) and the control group (n=16) received upper extremity exercises approximately 5 x 10-minute sessions per week for 4 weeks while also receiving standard upper limb care (including slings and supports). In addition, the treatment group (n=15) received static positioning of the affected arm in two different positions a day (1 lying, 1 sitting), each for 30 minutes per day, 5 days per week, for 4 weeks. The lying static position consisted of lying supine with the arm in comfortable full external rotation and 45° of abduction with elbow flexion. The sitting position consisted of sitting at a table, with both the shoulder and elbow in 90° flexion. Between-group post-scores showed significantly less development of external rotation shoulder contracture for the intervention group compared to the control group, as measured by a fluid-filled gravity goniometer.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static shoulder positioning of the hemiplegic arm during supine lying and sitting prevents external rotation shoulder contracture in patients witch acute stroke.
Shoulder flexion contracture
Not Effective
1B
One high quality RCT (Ada et al., 2005) examined the effect of positioning the affected shoulder in lying and in sitting for the prevention of shoulder flexion contracture in 31 patients with acute stroke. Both the intervention group (n=15) and the control group (n=16) received upper extremity exercises approximately 5 x 10-minute sessions per week for 4 weeks while also receiving standard upper limb care (including slings and supports). In addition, the treatment group (n=15) received static positioning of the affected arm in two different positions a day (1 lying, 1 sitting), each for 30 minutes per day, 5 days per week, for 4 weeks. The lying static position consisted of lying supine with the arm in comfortable full external rotation and 45° of abduction with elbow flexion. The sitting position consisted of sitting at a table, with both the shoulder and elbow in 90° flexion. No between-group difference was found for passive shoulder flexion contracture (measured by a fluid-filled gravity goniometer).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static shoulder positioning of the hemiplegic arm during supine lying and sitting does not prevent shoulder flexion contractures in patients witch acute stroke.
Shoulder pain
Not Effective
1B
One high quality RCT (Ada et al., 2005) examined the effect of positioning the affected shoulder in lying and in sitting for reducing pain in 31 patients with acute stroke. Both the intervention group (n=15) and the control group (n=16) received upper extremity exercises approximately 5 x 10-minute sessions per week for 4 weeks while also receiving standard upper limb care (including slings and supports). In addition, the treatment group (n=15) received static positioning of the affected arm in two different positions a day (1 lying, 1 sitting), each for 30 minutes per day, 5 days per week, for 4 weeks. The lying static position consisted of lying supine with the arm in comfortable full external rotation and 45° of abduction with elbow flexion. The sitting position consisted of sitting at a table, with both the shoulder and elbow in 90° flexion. No between-group difference was found for pain level on the Visual Analogue Scale.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static shoulder positioning of the hemiplegic arm during supine lying and sitting does not reduce shoulder pain in patients acute stroke.
Static arm positioning (without strapping) while lying or sitting – Subacute phase
Abduction contracture
Effective
1B
One high quality RCT (de Jong et al., 2006) have investigated the effects of static arm positioning in sitting and lying positions for reducing shoulder abduction contracture in patients with subacute stroke. This high quality RCT examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. At five weeks post treatment, there was significantly less shoulder abduction contracture in the experimental group, as measured by a masked fluid-filled goniometer, and significant improvements, as measured by the Fugl-Meyer Assessment for the upper extremity, in the ability to make selective movements with the affected arm when compared to the control group.
Note: 10 of the subjects from the experimental group went on to complete another 5 weeks of treatment – the data is not statistically analyzed in the paper and thus it was not included in this review.
Conclusions: There is moderate evidence (level 1b) from one high quality RCT that static positioning of the hemiplegic arm while in lying reduces shoulder abduction contracture in patients with subacute stroke.
External rotation contracture
Not Effective
1a
Two high quality RCTs (Dean et al., 2000, de Jong et al., 2006) have investigated the effects of static arm positioning in sitting and lying positions for decreasing shoulder external rotation contracture in patients witch subacute phase.
The first high quality RCT (Dean et al., 2000) investigated the effectiveness of three positions (2 lying, 1 sitting) to reduce shoulder pain and increase range of motion on the affected arm, combined with regular rehabilitation in 23 patients with subacute stroke. Patients were randomly assigned to a treatment group (n=10) or a control group (n=13). The intervention group received treatment daily for 6 weeks with each position being held for 20 minutes per day. For the first lying position, in supine, the shoulder was placed in maximal comfortable abduction and external rotation with the elbow flexed. The second lying position was in supine with the shoulder in 90° of abduction, maximal tolerable external rotation and elbow flexion. For the sitting position the shoulder was placed forward at 90° flexion, elbow and wrist in extension and a cylinder was placed in the hand to allow for web space stretch. The control group received typical multidisciplinary rehabilitation only. No significant between group differences were found post-intervention for passive external rotation contracture as measured by a standard goniometer and a gravity goniometer.
Note: As indicated by the authors, the study was insufficiently powered to provide conclusive results.
The second high quality RCT (de Jong et al., 2006) examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. No between-group difference was found for passive range of motion of shoulder external rotation, shoulder flexion, elbow extension or forearm supination as measured by a masked fluid-filled goniometer.
Note: 10 of the subjects from the experimental group went on to complete another 5 weeks of treatment – the data is not statistically analyzed in the paper and thus it was not included in this review.
Conclusions: There is evidence (level 1a) from two high quality RCTs that static positioning of the hemiplegic arm during supine lying and sitting does not decrease external rotation shoulder contracture in patients with subacute stroke.
Note: The reader is alerted that the sample sizes in both studies were small: thus they may not have been sufficiently powered (due to insufficient sample size) to find conclusive results. Hence we have indicated level 1a evidence but have removed the term strong that is usually associated with level 1a evidence.
Flexion contracture
Not Effective
1B
One high quality RCT (de Jong et al., 2006) have investigated the effects of static arm positioning in sitting and lying positions for decreasing flexion contracture in patients witch subacute phase. This high quality RCT examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. No between-group difference was found for shoulder flexion contracture as measured by a masked fluid-filled goniometer.
Note: 10 of the subjects from the experimental group went on to complete another 5 weeks of treatment – the data is not statistically analyzed in the paper and thus it was not included in this review.
Conclusions: There is moderate evidence (level 1b) from one high quality RCTs that static positioning of the hemiplegic arm during supine lying and sitting does not improve external rotation shoulder contracture in patients with subacute stroke.
Note: Sample size issues may have resulted in a study that was insufficiently powered to find significant difference.
Functional independence
Not Effective
1b
One high quality RCT (de Jong et al., 2006) have investigated the effects of static arm positioning in sitting and lying positions for improving functional independence in patients witch subacute phase. This high quality RCT examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. No between-group difference was found for functional independence as measured using the Barthel Index.
Note: 10 of the subjects from the experimental group went on to complete another 5 weeks of treatment – the data is not statistically analyzed in the paper and thus it was not included in this review.
Conclusions: There is moderate evidence (level 1b) from one high quality RCTs that static positioning of the hemiplegic arm during supine lying and sitting does not improve functional independence in patients with subacute stroke.
Note: Sample size issues may have resulted in a study that was insufficiently powered to find significant difference.
Range of motion of elbow extension and forearm supination
Not Effective
1B
One high quality RCT (de Jong et al., 2006) have investigated the effects of static arm positioning in sitting and lying positions for improving range of motion of elbow extension and forearm supination in patients witch subacute phase. This high quality RCT examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. No between-group difference was found for range of motion of elbow extension or forearm supination as measured by a masked fluid-filled goniometer.
Note: 10 of the subjects from the experimental group went on to complete another 5 weeks of treatment – the data is not statistically analyzed in the paper and thus it was not included in this review.
Conclusions: There is moderate evidence (level 1b) from one high quality RCTs that static positioning of the hemiplegic arm during supine lying and sitting does not improve range of motion of elbow extension or forearm supination in patients with subacute stroke. Note: Sample size issues may have resulted in a study that was insufficiently powered to find significant difference.
Shoulder pain
Not Effective
1A
Two high quality RCTs (Dean et al., 2000, de Jong et al., 2006) have investigated the effects of static arm positioning in sitting and lying positions, for prevention of shoulder pain in patients witch subacute stroke.
The first high quality RCT (Dean et al., 2000) investigated the effectiveness of three positions (2 lying, 1 sitting) to reduce shoulder pain and increase range of motion on the affected arm, combined with regular rehabilitation in 23 patients with subacute stroke. Patients were randomly assigned to a treatment group (n=10) or a control group (n=13). The intervention group received treatment daily for 6 weeks with each position being held for 20 minutes per day. For the first lying position, in supine, the shoulder was placed in maximal comfortable abduction and external rotation with the elbow flexed. The second lying position was in supine with the shoulder in 90° of abduction, maximal tolerable external rotation and elbow flexion. For the sitting position the shoulder was placed forward at 90° flexion, elbow and wrist in extension and a cylinder was placed in the hand to allow for web space stretch. The control group received typical multidisciplinary rehabilitation only. No significant between group differences were found post-intervention for pain while at rest or while dressing as measured by the Visual Analogue Scale.
Note: As indicated by the authors, the study was insufficiently powered to provide conclusive results.
The second high quality RCT (de Jong et al., 2006) examined the effectiveness of a contracture preventing arm positioning procedure (while lying supine) combined with traditional physical and occupational therapy treatment for 19 patients with subacute stroke and upper limb hemiplegia. Individuals in the experimental group (n=10) were positioned while lying supine with their affected arm in maximum comfortable shoulder abduction, external rotation, elbow extension and supination of the forearm without pain for 5 weeks, 2 x 30-minute sessions per day, five days per week, in addition to conventional rehabilitation. The arm was supported by a pillow and maintained in the position using a sandbag. The control group (n=9) received conventional rehabilitation only. No between-group difference was found for pain at the end range of passive motion.
Note: 10 of the subjects from the experimental group went on to complete another 5 weeks of treatment – the data is not statistically analyzed in the paper and thus it was not included in this review.
Conclusions: There is evidence (level 1a) from two high quality RCTs that static positioning of the hemiplegic arm during supine lying and sitting does not reduce pain in patients with subacute stroke.
Note: The reader is alerted that the sample sizes in both studies were small: thus they may not have been sufficiently powered (due to insufficient sample size) to find conclusive results. Hence we have indicated level 1a evidence but have removed the term strong that is usually associated with level 1a evidence.
Note: Again sample size issues may have resulted in a study that was insufficiently powered to find significant difference.
Static arm positioning (without strapping) while lying or sitting – Chronic phase
External shoulder rotation contracture
Not Effective
1B
One high quality RCT (Gustafsson & McKenna, 2006) examined the effectiveness of positioning the affected arm in 2 static positions (1 sitting, 1 lying) for decreasing external shoulder rotation contracture in 32 patients with chronic stroke. Individuals in the intervention group (n=17) received static positioning treatment 2 x 20-minute sessions per day for 4 weeks. Lying in supine, the individual’s affected arm was placed in 90° shoulder abduction, maximal comfortable external rotation, elbow flexion and supination for 20 minutes daily over 4 weeks. As well, whenever lying in bed and not placed in this static position, the patients in the intervention group used a pillow to support the affected arm in a position midway between external and internal rotation and not horizontally adducted. During sitting, individuals in the intervention group had their shoulder supported in 90° abduction with elbow extended and forearm in neutral for 20 minutes daily over 4 weeks. As well, whenever the patients in the intervention group were in a sitting position over the four-week period (when not in static position), their affected arm was positioned, using a Otto Bock modular arm rest support attached to the arm of their wheelchair, alongside the trunk in 10-15° of shoulder abduction and midway between external and internal rotation. Individuals in the control group (n=15) received locally fabricated cushion supports for their affected upper limb when seated and when in bed. The results revealed no significant between group difference for external shoulder rotation contracture as measured by a universal goniometer.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static positioning of the hemiplegic arm during supine lying and sitting does not decrease external rotation shoulder contracture in patients with chronic stroke.
Functional independence
Not Effective
1B
One high quality RCT (Gustafsson & McKenna, 2006) examined the effectiveness of positioning the affected arm in 2 static positions (1 sitting, 1 lying) for improving functional independence 32 patients with chronic stroke. Individuals in the intervention group (n=17) received static positioning treatment 2 x 20-minute sessions per day for 4 weeks. Lying in supine, the individual’s affected arm was placed in 90° shoulder abduction, maximal comfortable external rotation, elbow flexion and supination for 20 minutes daily over 4 weeks. As well, whenever lying in bed and not placed in this static position, the patients in the intervention group used a pillow to support the affected arm in a position midway between external and internal rotation and not horizontally adducted. During sitting, individuals in the intervention group had their shoulder supported in 90° abduction with elbow extended and forearm in neutral for 20 minutes daily over 4 weeks. As well, whenever the patients in the intervention group were in a sitting position over the four-week period (when not in static position), their affected arm was positioned, using a Otto Bock modular arm rest support attached to the arm of their wheelchair, alongside the trunk in 10-15° of shoulder abduction and midway between external and internal rotation. Individuals in the control group (n=15) received locally fabricated cushion supports for their affected upper limb when seated and when in bed. The results revealed no significant between group difference for functional independence using the modified Barthel Index.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static positioning of the hemiplegic arm during supine lying and sitting does not improve functional independence in patients with chronic stroke.
Motor activity
Not Effective
1B
One high quality RCT (Gustafsson & McKenna, 2006) examined the effectiveness of positioning the affected arm in 2 static positions (1 sitting, 1 lying) for improving motor activity in 32 patients with chronic stroke. Individuals in the intervention group (n=17) received static positioning treatment 2 x 20-minute sessions per day for 4 weeks. Lying in supine, the individual’s affected arm was placed in 90° shoulder abduction, maximal comfortable external rotation, elbow flexion and supination for 20 minutes daily over 4 weeks. As well, whenever lying in bed and not placed in this static position, the patients in the intervention group used a pillow to support the affected arm in a position midway between external and internal rotation and not horizontally adducted. During sitting, individuals in the intervention group had their shoulder supported in 90° abduction with elbow extended and forearm in neutral for 20 minutes daily over 4 weeks. As well, whenever the patients in the intervention group were in a sitting position over the four-week period (when not in static position), their affected arm was positioned, using a Otto Bock modular arm rest support attached to the arm of their wheelchair, alongside the trunk in 10-15° of shoulder abduction and midway between external and internal rotation. Individuals in the control group (n=15) received locally fabricated cushion supports for their affected upper limb when seated and when in bed. The results revealed no significant between group difference for motor recovery as measured by the Motor Assessment Scale.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static positioning of the hemiplegic arm during supine lying and sitting does not improve motor activity in patients with chronic stroke.
Shoulder pain
Not Effective
1B
One high quality RCT (Gustafsson & McKenna, 2006) examined the effectiveness of positioning the affected arm in 2 static positions (1 sitting, 1 lying) for decreasing shoulder pain in 32 patients with chronic stroke. Individuals in the intervention group (n=17) received static positioning treatment 2 x 20-minute sessions per day for 4 weeks. Lying in supine, the individual’s affected arm was placed in 90° shoulder abduction, maximal comfortable external rotation, elbow flexion and supination for 20 minutes daily over 4 weeks. As well, whenever lying in bed and not placed in this static position, the patients in the intervention group used a pillow to support the affected arm in a position midway between external and internal rotation and not horizontally adducted. During sitting, individuals in the intervention group had their shoulder supported in 90° abduction with elbow extended and forearm in neutral for 20 minutes daily over 4 weeks. As well, whenever the patients in the intervention group were in a sitting position over the four-week period (when not in static position), their affected arm was positioned, using a Otto Bock modular arm rest support attached to the arm of their wheelchair, alongside the trunk in 10-15° of shoulder abduction and midway between external and internal rotation. Individuals in the control group (n=15) received locally fabricated cushion supports for their affected upper limb when seated and when in bed. The results revealed no significant between group difference on shoulder pain as measured by the Ritchie Articular Index and the Visual Analogue Scale.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that static positioning of the hemiplegic arm during supine lying and sitting does not decrease shoulder pain in patients with chronic stroke.
Body positioning during lying
Lying on the unaffected vs. affected side for optimal rehabilitation outcomes
Insufficient Evidence
5
Three surveys (Chatterton et al., 2001, Rowat, 2001, Mee & Bee, 2007) investigated clinician preferences for whether a patient should lie on the affected vs. unaffected side for optimal rehabilitation.
The first survey by Chatterton et al. (2001) of 436 physiotherapists found that 97% recommended side lying on the non-affected side post-stroke and 92% side lying on affected side. 85% “frequently recommended” side lying on the unaffected side while 66% “frequently recommended” side lying on the affected side. Sitting in an armchair was recommended by 98%.
The second survey by Rowat (2001) of nurses and five other disciplines examined preferred practice in positioning post-stroke. 80% of clinicians indicated that the best position for an unconscious patient was lying on the non-affected side to encourage functional recovery of the paretic side and avoid complications such as pressure sores. There was a lack of consensus on the effectiveness of other positions including positioning on the affected side in conscious or unconscious patients.
The third survey by Mee & Bee, (2007) surveyed nurses, physiotherapists and occupational therapists in Singapore hospitals. Most indicated that they perceived that the best position for an unconscious patient with stroke and hemiplegia was side lying on the unaffected side. However, nurses working on a neurology ward perceived that supine lying with 30o angle was the best position.
Conclusion: There is insufficient scientific evidence (level 5) indicating whether lying on the affected or unaffected side is best for optimal stroke rehabilitation. However three surveys found that clinicians prefer their patients who have had a stroke to be positioned on their unaffected side.
Lying supine propped up at an angle vs. side lying (affected or unaffected side) and lying flat supine for optimal arterial O2 saturation
Conflicting
4
One case-control study (Elizabeth et al., 1993) and one repeated measures study (Chatterton et al., 2000) examined whether side lying vs. flat supine lying vs. lying propped up at an angle is the most effective for optimal arterial O2 saturation.
The case-control study by Elizabeth et al. (1993) examined arterial oxygen saturation in 10 patients with acute stroke positioned for one hour in the following positions (in a set sequence): lying supine, lying on the right side, lying on the left side and lying propped up at 45° compared to a matched control group (n=10), of patients with other medical conditions. When in side lying and flat supine positions, mean O2 saturation was significantly lower in the patients with stroke than the controls, however when patients were propped at 45°, the group difference was not significant. The findings suggest that it may be beneficial for patients to be propped up while lying during acute stroke rehabilitation, to reduce the blood flow to the dependent lung that often results from side lying (especially when lying on the affected side) thus preventing hypoxemia.
The repeated-measures study by Chatterton et al. (2000) examined the within-subject difference in arterial oxygen saturation of 24 patients with acute stroke who spent 1 hour in various positions – lying on affected side with the head of the bed at a 45° incline, lying on unaffected side at 45° incline, sitting up in bed inclined at 70° and sitting in an armchair. There were no significant differences in oxygen saturation values between any of the positions and saturation values were maintained at acceptable values while the subject was lying on the affected side or the unaffected side while the bed was inclined at 45°.
Note: The affected shoulder while lying on the affected side was flexed with the scapula protracted and the affected shoulder while lying on the unaffected side was slightly flexed with scapula in neutral and the unaffected shoulder flexed with scapula protracted.
Conclusion: There is conflicting evidence (level 4) between one case-control study that found that positioning a patient with acute stroke in bed in a propped supine lying position at a 45° allows for significantly more 02 saturation than positioning the patient in a side lying position (affected or unaffected side) and one repeated measures clinical study that found no difference in 02 saturation in patients with acute stroke who were positioned in side lying (affected or unaffected side) at 45° vs. lying supine and propped up at an angle of 70° vs. sitting fully upright.
Supine lying on a bed positioned flat (i.e. 0 degrees) vs. lying propped up at an angle for optimal blood flow velocity
Effective
2b
Two studies used a repeated measures design (Wojner et al., 2002, Wojner et al., 2005) examined the effect of different angles of supine lying on blood flow velocity in patients with acute stroke.
The first repeated measures cross-over study (Wojner et al., 2002) examined the effect of three positions on middle cerebral artery mean flow velocities (measured with Transcranial Doppler sonogrophy) in 11 patients with acute ischemic stroke. Measurements were made over a single session of unspecified length at 30°, 15°, 0° head of bed angle, with a 2 minutes stabilization period between angle change and measurement. Mean flow velocity increased significantly when the head of bed was lowered to flat position (0°) compared to the 2 other angles. Mean arterial pressure, heart pulse and pulse pressure remained stable. Findings from this small sample suggest that patients with acute ischemic stroke would benefit from a flat position as it promotes an increase in flow to ischemic brain tissue.
The second repeated measures cross-over study (Wojner et al., 2005) investigated the effect of bed positioning on residual blood flow velocity in acutely occluded arteries in 20 patients with acute stroke. The middle cerebral artery mean flow velocity in twenty patients with acute (< 24 hours) ischemic stroke was measured with Transcranial Doppler sonogrophy, over a single session of an unspecified length with the head of the patient’s bed positioned at 0°, 15° and 30°, with a 15 minute stabilization period between angle change and measurement. Mean flow velocity increased in all patients after lowering to 0° but no change was noted in mean arterial pressure, pulsatility index and heart rate. Results indicated that patients with acute ischemic stroke may benefit from flatter head of bed positioning as it promotes residual blood flow to ischemic brain tissue.
Conclusion: There is limited evidence (level 2b) from two repeated measures studies that lying supine in bed with the head of the bed flat (i.e. 0°) is the most optimal position for enhancing blood flow to the brain for patients with acute ischemic stroke.
Upper extremity positioning in sitting
Positioning arm in trough or lap tray to prevent/reduce shoulder subluxation
Conflicting
4
Two repeated measures studies (Moodie et al., 1986, Brooke et al., 1991) investigated the effectiveness of arm troughs and lap trays for preventing shoulder subluxation during chair/wheelchair sitting.
One repeated measures study (Moodie et al., 1986) examined the effectiveness of five supportive devices during sitting (conventional triangular sling, the Bobath shoulder roll, the Hook-Hemi Harness, the plexiglass lap tray and the arm trough) for managing hemiplegic shoulder subluxation in 10 individuals with subacute stroke. Degree of subluxation was determined in this study by comparing the width of glenohumerol space in the affected shoulder vs. the unaffected shoulder. The study took place over a 45-minute session and involved 7 x-rays per participant. First the unaffected shoulder was x-rayed as a control, followed by the affected shoulder (unsupported) and finally the affected shoulder was x-rayed while supported by each of the 5 support devices. Results indicated a significant reduction in shoulder subluxation for the devices meant for use while chair/wheelchair sitting (the plexiglass lap tray and the arm trough).
Note: Moodie et al. also mention in their study that the arm trough immobilized the affected limb, unnecessarily limiting sensory and motor input. In contrast the lap tray allows bilateral activities to occur.
A second repeated measures study (Brooke et al., 1991) examined the effect of three shoulder supports (Harris Hemisling, the Bobath sling, and the arm trough or lap board) on hemiplegic shoulder subluxation in individuals (n= 10) following some type of recent brain damage (6 had ischemic infarcts). The lap tray was used in certain conditions instead of the arm trough such as when the arm was not adequately placed in the latter support. The study used x-ray to measure for subluxation. Regarding the supports meant for use while sitting (arm trough or lap board), results showed that they tended to overcorrect for vertical subluxation and correct well for horizonal subluxation. The authors also stated that the use of an arm trough decreased shoulder adduction and internal rotation and facilitated independent transfers compared to a lapboard.
Note: Boyd et al. (1999) compared the results of two surveys done in 1984 and 1994 to investigate frequency of use and intended purpose of arm supports post-stroke. Occupational therapists and other rehabilitations staff at facilities listed in the Canadian Hospital directory completed the questionnaires. The lapboard and arm trough were two of the three most frequently used supports at both given times. Also at both times, the most frequent reason chosen to use a lapboard was to increase awareness of the arm. Similarly the main reason chosen to use an arm trough was to protect the arm. However, these 2 reasons for using the devices were chosen notably less in 1994 then they were in 1984.
Conclusion: There is conflicting evidence (level 4) between two repeated measures studies, with one of study finding that arm troughs and lapboards correctly reduce subluxation for patients with stroke and the other finding that arm troughs and lapboards tend to overcorrect subluxation for patients with stroke.
Static positioning of the affected arm while ambulating to reduce shoulder subluxation
Effective
2b
Three repeated measures studies (Zorowitz et al., 1995, Moodie et al., 1986, Brooke et al., 1991) one quasi-experimental study (Hurd et al., 1974) and one survey (Foongchomcheay et al., 2005) examined the effectiveness of using supports for the reduction of shoulder subluxation in patients with subacute stroke as measured by x-ray over a single session.
The first repeated measures study (Zorowitz et al., 1995) examined the effectiveness of 4 supports (single-strap hemisling, Bobath Roll, Rolyan humeral cuff and Cavalier support) for reducing shoulder subluxation in 20 patients with subacute stroke. The study took place over one session and involved 6 separate x-rays. First the unaffected shoulder was x-rayed for use as a control, followed by the affected shoulder (unsupported) and finally the affected shoulder was x-rayed while supported by each of the 4 slings/supports. The results indicated that vertical subluxation was virtually eliminated by the use of the single-strap hemisling. As well, the Rolyan humeral cuff sling was found to significantly reduce total subluxation asymmetry compared to wearing no sling. No significant pre-post differences were found for the Bobath Roll or the Cavalier support.
The second repeated measures study (Moodie et al., 1986) investigated the effects of using 5 different shoulder supports (conventional triangular sling, Bobath roll, Hook-Hemi harness, plexiglass lap tray and arm trough) on reducing shoulder subluxation in clients with stroke during the subacute phase. The study involved 10 individuals with subacute stroke who received 7 x-rays over a 45-minute session. First the unaffected shoulder was x-rayed as a control, followed by the affected shoulder (unsupported) and finally the affected shoulder was x-rayed while supported by each of the 5 support devices. Regarding the devices meant for use while ambulating (i.e. the conventional triangular sling, Bobath roll and Hook-Hemi harness) a significant reduction in shoulder subluxation was found for the conventional triangular sling only, measured by comparing the x-rays of before and during use of the device. The authors concluded however, that although the conventional triangular sling may reduce shoulder subluxation, it did not fulfill some other requirements of upper extremity positioning, primarily the reinforcement of spastic flexor pattern.
A third repeated measures study (Brooke et al., 1991) examined the effect of three shoulder supports (Harris hemisling, the Bobath sling, and the arm trough or lap board) on hemiplegic shoulder subluxation in individuals (n= 10) following some type of recent brain damage (6 had ischemic infarcts). The lap tray was used in certain conditions instead of the arm trough such as when the arm was not adequately placed in the latter support. The study used x-ray to measure for subluxation. Regarding the supports meant for use while ambulating (Harris hemisling and Bobath sling), results showed that both the supports corrected subluxation notably, however the Bobath sling was more variable in it’s effectiveness, caused problems (distracted the glenhumeral joint horizontally) and was significantly less effective at correcting subluxation compared to the Harris hemisling.
One quasi-experimental study (Hurd et al., 1974) investigated the effectiveness of using a hemisling to reduce shoulder subluxation and pain in 14 patients with acute stroke. Individuals in the experimental group (n=7) wore the hemisling following initial assessment and were evaluated approximately 2-3 weeks later, and assessed again at 3-7 months post stroke. The control group (n=7) wore no sling for the whole time period. No appreciable between group differences were found for shoulder subluxation, pain, range of motion or peripheral nerve injuries. It is to be noted that the outcome measures are not clearly outlined in the study nor is it stated whether or not any blinding took place.
In the survey, Foongchomcheay et al. (2005) investigated the practices of 210 hospitals in Australia on the devices they use to prevent shoulder subluxation after stroke. Findings indicated that the majority of physiotherapists prescribed slings (collar and cuff) for shoulder subluxation and inadequate arm strength, to be worn at all times out of bed to help prevent shoulder subluxation.
Conclusion: There is limited evidence (level 2b) from three repeated measures studies that wearing certain types of slings and supports significantly reduces shoulder subluxation while wearing the support. Specifically, one of the studies found that a single strap sling eliminates vertical subluxation, a Rolyan humeral cuff significantly reduces total shoulder subluxation and the Bobath roll and the Cavalier support do not reduce subluxation, the second repeated measures study found that the triangular sling but not the Bobath roll or Hook-Hemi harness improves shoulder subluxation, and the third repeated measures study found that the Harris hemisling reduces vertical and horizontal subluxation significantly better than the Bobath sling. One poorly designed quasi-experimental study found that a hemisling does not improve subluxation, pain or range of motion over a 6-month period.
Note: The quasi-experimental study was likely insufficiently powered, because of a small sample size, to detect anything other than large differences. Finally, one survey found that the majority of clinicians recommend slings to be worn at all times.
Static positioning of the affected arm while sitting in a chair to encourage reflex inhibiting patterns of posture
Insufficient Evidence
5
A review of the literature on stroke patient care identified the recommended postures and the rational behind using these postures for individuals with stroke (Carr & Kenney, 1992). As for the upper extremity while sitting in a chair, all sources agreed to place the shoulder in protraction with the arm brought forward, the wrist in neutral with fingers extended and thumb abducted. An inference was made that the following should be avoided: shoulder extension, adduction and internal rotation; however the recommended amount of shoulder flexion, abduction and external rotation varied as well as the height and number of pillows or tables to support the affected arm. There were two main “schools of thought” where some had the arm straight forward and others had the arm in slightly abduction and external rotation. One of the sources mentioned that both positions were advantageous. For positioning of the elbow there were two “school of thoughts” once again. One was to place the elbow in full extension and the other was to place the elbow in slight flexion. Regarding the hand, the majority opinion was to place the hand in pronation, whether sitting in a chair, or sitting in bed.
Conclusion: While there is insufficient scientific evidence (level 5) that arm positioning during chair-sitting can improve reflex inhibiting postural patterns, one review of the literature on stroke patient care concluded that positioning the affected upper limb while sitting in a chair in shoulder protraction and arm forward, hand pronated, wrist neutral, fingers extended and thumb abducted can encourage reflex-inhibiting patterns in individuals following a stroke.
Static positioning of the affected arm while sitting in bed to encourage reflex inhibiting patterns of posture
Insufficient Evidence
5
Carr & Kenney (1992) conducted a review of the literature on recommended stroke patient care to identify the optimal position in order to maintain a reflex inhibiting pattern of posture while sitting in bed. The general consensus of the optimal sitting position was as follows: The patient is in an upright position with the head and trunk in midline position. The affected shoulder is in protraction and arm is forward and flex while supported by a pillow. A pillow also supports the trunk. Legs are to be straight and not externally rotated. There is still controversy concerning shoulder abduction in sitting position in bed. Regarding the hand, the majority opinion was to place the hand in pronation, whether sitting in a chair, or sitting in bed. Note: there was no study evaluating the exact benefits of this recommended position.
Conclusion: While there is insufficient scientific evidence (level 5) that arm positioning during bed-sitting can improve reflex inhibiting patterns of posture, one literature review concluded that sitting upright, with head and trunk in midline position, shoulder in protraction and the arm forward and flexed, and legs straight is the most optimal position for improving reflex inhibiting patterns of posture.
Upper extremity positioning during transfers
Positioning of arm while transferring from sitting to standing to prevent/reduce shoulder subluxationInsufficient Evidence
Insufficient Evidence
5
One literature review (Seneviratne et al., 2005) examined the current best practice in prevention and treatment of shoulder subluxation and found that the arm must always be supported during transfers in order to avoid glenohumeral subluxation. However, the review revealed a lack of consensus of best practice regarding positioning and transferring in general.
Conclusion: There is insufficient scientific evidence (level 5) regarding whether position handling while transferring from sit to stand has an effect on shoulder subluxation and pain. However, one literature review recommends that the hemiplegic arm should always be supported while transferring the patient from sitting to standing.
Note: While the scientific evidence does not reveal any RCTs it is likely that this type of study is not doable because best practices already recognize the need for support of the arm during transfers.
Positioning of arm while turning in bed to prevent/reduce shoulder subluxation and pain
Insufficient Evidence
5
One literature review (Gilmore et al., 2004) examined the possible causes of shoulder pain and discussed the implications for occupational therapy treatment including handling the patient. The authors stated that, when turning a patient, it is essential that the affected arm be supported and the trunk brought forward by grasping behind the scapula and not pulling on the affected arm. Pulling on the arm could cause trauma or subluxation.
Conclusion: There is insufficient scientific evidence (level 5) regarding whether position handling while turning in bed has an effect on shoulder subluxation and pain. However, one literature review found that carers should grasp behind the scapula when turning the patient in bed.
Note: While the scientific evidence does not reveal any RCTs it is likely that this is because best practices already recognize the need for support of the arm during turning in bed.
References
Ada L., Goddard E., McCully J., & Bampton J. (2005). Thirty minutes of positioning reduces the development of shoulder external rotation contracture after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 86(2): 230-34.
Boyd E.A., Pepin P., & Szabo-Hartin J. (1999). Shoulder supports revisited: A Canadian follow-up survey. Canadian Journal of Occupational Therapy, 66(4): 161-68.
Brooke M.M., de Lateur B.J., Diana-Rigby C.G., & Questad K.A.(1991). Shoulder Subluxation in HemiplegiaComplete paralysis of the arm, leg, and trunk on one side of the body that results from damage to the parts of the brain that control muscle movements. Hemiplegia is not a progressive condition, nor is it a disease.: Effects of Three Different Supports. Archives of Physical Medicine and Rehabilitation, 72: 582-86.
Carr E.K., & Kenney F.D. (1992). Positioning of the strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patient: a review of the literature. International Journal of Nursing Studies, 29: 355-369.
Chatterton H.J., Pomeroy V.M., & Gratton, J. (2001). Positioning for strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients: a survey of physiotherapists aims and practices. Disability and Rehabilitation, 23(10), 413-421.
Chatterton H.J., Pomeroy V.M., Connolly M.J., Faragher E.B., Clayton L., & Tallis, R.C. (2000). The effect of body position on arterial oxygen saturation in acute strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Journal of gerontology, 55A(4); M239-M244.
De Jong L.D., Nieuwboer A., & Aufdemkampe, G. (2006). Contracture preventive positioning of the hemiplegic arm in subacute strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients: a pilot randomized controlled trial. Clinical Rehabilitation, 20: 656-667.
Dean C.M., Mackey F.H., & Katrak P. (2000). Examination of shoulder positioning after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: A randomized controlled pilot trial. Australian Journal of Physiotherapy, 46:35-40.
Elizabeth J., Singarayar J., Ellul J., Barer D., & Lye M. (1993). Arterial oxygen saturation and posture in acute strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Age & Ageing, 22(4):269-72.
Foongchomcheay A., Ada L., & Canning C. (2005). Use of devices to prevent subluxation of the shoulder after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Physiotherapy Research International 10: 134-145.
Gilmore P.E., Spaulding S.J., & Vandervoort A.A. (2004). Hemiplegic shoulder pain: Implications for occupational therapy treatment. The Canadian Journal of Occupational Therapy, 71(1): 36-46.
Gustafsson L., & McKenna K. (2006). A program of static positional stretches does not reduce hemiplegic shoulder pain or maintain shoulder range of motion-a randomized controlled trial. Clinical Rehabilitation, 20:277-86.
Hurd M., Farrel K., &Waylonis G. (1974). Shoulder Sling for HemiplegiaComplete paralysis of the arm, leg, and trunk on one side of the body that results from damage to the parts of the brain that control muscle movements. Hemiplegia is not a progressive condition, nor is it a disease.: Friend or Foe? Archives of Physical Medicine and Rehabilitation, 55: 519-522.
Mee L.Y., & Bee W.H. (2007). A comparison study on nurses’ and therapists’ perception on the positioning of strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients in Singapore General Hospital. International Journal of Nursing Practice, 13(4): 209-21
Mee L.Y., & Bee W.H. (2007). A comparison study on nurses’ and therapists’ perception on the positioning of strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients in Singapore General Hospital. International Journal of Nursing Practice, 13(4): 209-21.
Moodie N.B., Brisnin J., & Morgan A.M.G. (1986). Subluxation of the glenohumeral joint in hemiplegiaComplete paralysis of the arm, leg, and trunk on one side of the body that results from damage to the parts of the brain that control muscle movements. Hemiplegia is not a progressive condition, nor is it a disease.: Evaluation of supportive devices. Physiotherapy Canada, 38 (3): 151-57.
Rowat A.M. (2001). What do nurses and therapists think about the positioning of strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients? Journal of Advanced Nursing, 34(6): 795-803.
Seneviratne C., Then K.L., Reimer, M. (2005). Post-stroke shoulder subluxation: a concern for neuroscience nurses. AXON, 27(1): 26-31.
Wojner A.W., El-Mitwalli A., & Alexandrov A.V. (2002). Effect of Head positioning on intracranial blood flow velocities in acute ischemic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a pilot study. Critical Care NurseIn charge of, but not limited to, the "assessment and provision of care needs; support and education for patients and families; discharge planning."(Suggested by Philips et al, 2002) , 24(4): 57-66.
Wojner A.W., Garami Z., Chenyshev O.Y., & Alexandrov A.V. (2005). Head down: flat positioning improves blood flow velocity in acute ischemic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. American Academy of Neurology, 64: 1354-1357.
Zorowitz R.D., Idank D., Ikai T., Hughes M.B., & Johnson M.V. (1995). Shoulder Subluxation After StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: A comparison of four Supports. Archives of Physical Medicine and Rehabilitation, 76: 763-771.
Manage Cookie Consent
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.