Introduction
Robot-assisted upper extremity training consists of repetitive practice of goal-directed exercises and activities of the upper extremities using a robot device/system. Robot-assisted upper extremity training is offered with the goal to improve upper extremity function post-stroke and can be used in acute, subacute and chronic stages of stroke recovery. Participants typically engage in functional exercises in different modes (e.g. passive, passive-assisted, active) that involve different muscle groups (e.g. shoulder and elbow vs. wrist and fingers), and perform exercises in horizontal and/or vertical positional planes.

Please click here to visualise the following table in a pdf.
| Device | Target | Motion Type | Feedback | Degree Of Freedom | Type Of Exercise | Design |
| Active Joint Brace for the Elbow | Proximal | Active assistance | Kinesthetic, proprioceptive, tactile and visual sensory. | N/A | Elbow flexion and extension in a set of functionally oriented tasks tailored to each subject’ motor abilities. | Mobile exoskeleton EMG-controlled powered |
| ARMGuide | Proximal | Active-assisted | Graphical feedback of the hand position and feedback on the amount of motor assistance. | 3 | Reaching movements in different directions | Singly-actuated
 |
| ARMin I and ARMin II | Proximal and distal | Passive and active | Visual and auditory | 6 independently actuated DOF and 1 coupled DOF | Functional 3D workspace repetitive exercises | Exoskeleton
 |
| BATRAC | Proximal | Passive | Auditory | N/A | Push and pull exercises in bilateral mode | End-effector
http://medicalxpress.com/news/2011-09-rewiring-brain-regain.html
 |
| BFIAMT | Proximal | Bilateral active passive, bilateral reciprocal, bilateral passive, bilateral symmetric. | Visual | N/A | Push and pull exercises. | End-effector |
| Bilateral Forearm and Wrist Trainer | Distal | Passive, active. | N/A | 1 | Supination movement of forearm and dosiflexion/volarflexion of the wrist, bimanual, repetitive practice. | End-effector |
| Bi-Manu-Track | Distal | Passive-passive, passive-active, active-active. | Visual | 1 | Bilateral elbow pronation and supination, wrist flexion and extension in a mirror or parallel fashion. | End-effector
http://www.reha-stim.de/cms/index.php?id=60
 |
| Braccio di Ferro | Proximal | Adaptive control of robot assistance | Visual position of the hand and target, haptic feedback. | 2 | Shoulder and elbow movement in horizontal plane in a goal directed activity. | Actuated
http://www.redorbit.com/news/technology/1836376/robot_teaches_stroke_survivors/
 |
| GENTLE/S | Proximal | Passive, active assisted or active. | Virtual reality haptic interface. | 3 | Hand to mouth movements, reaching movements. | Exoskeleton
http://www.mimics.ethz.ch/index.php?page_id=2
 |
| HandCare | Distal | Assisted | Visual | 5 | Opening and closing movements in a goal directed exercises. | End-effector |
| HapticKnob | Distal | Assisted, resistive | Interactive and intuitive visual feedback. | 2 | Grasping in coordination with pronation/supination of the forearm. | End-effector
http://www.sciencedirect.com/science/article/pii/S0924424710000154
 |
| HWARD | Distal | Assisted, active assisted. | Visual and auditory. | 3 | Grasp and release movements in a virtual-environment (VR) setting. | Pneumatically actuated |
| L-EXOS | Proximal | Active assisted. | Force feedback, visual feedback , auditory cueing during tasks. | 5 | VR environment reaching, path following and free motion exercises. | Exoskeleton |
| MEMOS | Proximal | Active, passive, active-assisted, resistive. | Visual feedback of the current position of the handle was provided. | N/A | Elbow and shoulder exercises in a sequence point-to-point reaching movements in the horizontal plane. | Actuated, end-effector. |
| MIME | Proximal | Passive, active –assisted, active-constrained, bilateral modes | Feedback of the fraction of the movement completed or the time to complete was used to track and motivate performance. | 6 | Unilateral or bilateral shoulder and elbow movement in target reaching activities. | Exoskeleton
http://www.rehab.research.va.gov/j
 |
| MIT-Manus | Proximal | Assisted | Visual, auditory, and tactile | 2 | Shoulder and elbow movement in horizontal plane, repetitive reaching exercises. | Exoskeleton
http://www.techshout.com/science/2010/17/mit-manus-robot-assisted-therapy-may-help-stroke-patients-regain-function/
 |
| Proximal and distal | Assisted, resistive, passive. | | 3 | Abduction/adduction, flexion/extension, pronation/supination, vertical movements, grasping exercises. | Exoskeleton | |
| NeReBot | Proximal | Assisted. | Visual and auditory. | 3 | Flexion and extension, pronation and supination, adduction and abduction, circular movements of shoulder and elbow. | Direct drive wire actuation, can be used in sitting or lying positions.
http://www.mechatronics.it/index.php?lingua=ENG&pag=res&sub=att&id=16
 |
| Pneumatic Glove | Distal | Assisted, assist as needed. | Haptic, visual . | 5 | Grasp release tasks, digit extension with VR environment and real objects. | Exoskeleton |
| ReoGo | Proximal | Passive, active, active assisted. | Visual and auditory. | N/A | Reaching objectives on the computer screen using elbow and shoulder joints, in 3 dimensions and on all spatial planes. | End-effector |
| REHAROB Therapeutic System | Proximal | Passive assistance | N/A | N/A | Shoulder and elbow physiotherapy, executing exercises slowly and with constant velocity in a high repetition number.
 | Exoskeleton
http://www.a1tech.hu/reharob_en.htm |
| Robot-Assisted Individualized Finger Rehabilitation | Distal | Full passive, assisted. | N/A | N/A | Simulated grasping and releasing training, VR based recreational activity. | End -effector |
| T-WREX and Pneu-WREX | Proximal and distal | Passive (non-robotic) arm orthosis that provides support for the arm against gravity | Auditory and visual feedback, objective feedback of task performance at end of each game. | 5 | Functional exercises in 3D/Virtual environment tasks, repetitive. | Exoskeleton
http://www.ric.org/research/centers/mars3/archives/mars-rerc/twrexdesc/
 |
| Proximal | Assist as needed | Auditory and visual | 4 | Elbow flexion/extension, shoulder horizontal abduction/adduction, shoulder flexion/extension, and forward/backward translation , functional 3D tasks | Exoskeleton
http://www.readcube.com/articles/10.1186/1743-0003-6-20 |  |
Clinician Information
Note: When reviewing the findings, it is important to note that they are always made according to randomized clinical trial (RCT) criteria – specifically as compared to a control group. To clarify, if a treatment is “effective” it implies that it is more effective than the control treatment to which it was compared. Non-randomized studies are no longer included when there is sufficient research to indicate strong evidence (level 1a) for an outcome.
The current module reviewed 47 studies (16 high quality RCTs, four fair quality RCTs, one poor quality RCT and 26 non-randomized studies) that have investigated robot-assisted upper extremity (UE) training. Robot-assisted UE training typically included goal-directed functional tasks relating to UE movements of the shoulder, elbow, wrists and digits. Frequency of robot-assisted UE training varied from 10 to 60-minutes per session, 3 to 5 times a week for 4 to 11 weeks period. Control groups included conventional UE training, sham robot-assisted therapy, sling suspension, neurodevelopmental therapy, task-matched unassisted therapy, or no rehabilitation to the affected hand. A recent Cochrane review (Mehrholz et al., 2012) that comprised 19 RCTs or controlled clinical trials (13 of which were reviewed and included in this Stroke Engine module) reported statistically significant differences in favour of robot-assisted UE training compared to control interventions in activities of daily living and arm function, but not in muscle strength. The authors report that results should be interpreted with caution given variations in duration of training, type of device used and patient characteristics. In fact, a recent systematic review (Norouzi-Geidari et al., 2012) which included 12 RCTs (all of which were included in this Stroke Engine module and in the review by Mehrholz et al., 2012) reports no significant differences between the robot-assisted UE training and conventional therapy in motor recovery, activities of daily living, strength and motor control when the duration/intensity of both interventions is matched. To draw clear results on the effectiveness of robot-assisted therapy in comparison to conventional care, this Stroke Engine module includes studies in which robot-assisted UE training was compared to conventional rehabilitation of similar intensity or no rehabilitation. Accordingly, studies that compared robot-assisted UE training with another intervention such as functional electrical stimulation or neuromuscular stimulation have not been included in this module at this stage. Further, given the numerous differences in duration/intensity of treatment, types of device and exercises used, this module presents outcomes specific to each device/system studied. Overall, different types of robot-assisted UE training have been found to be effective for improving various UE outcomes across the continuum of stroke recovery. In the acute phase of stroke recovery, the NeReBot has been shown to be more effective than comparison interventions for improving functional independence and UE function. In the subacute stage of recovery the MIME has been shown to be more effective than comparison interventions for improving UE function. In the chronic stage of recovery the BATRAC system has been shown to be more effective than comparison interventions for improving range of motion and UE function; the Bi-Manu-Track system is more effective than comparison interventions for improving UE function and UE motor activity; the GENTLE/S is more effective than comparison interventions for improving UE function; and the MIME is more effective than comparison interventions for improving kinematics, strength and UE function. Other robotic devices used in the chronic stage of stroke recovery have also been shown to cause significant improvements in UE outcomes, although their effectiveness compared with a control or comparison intervention has not yet been performed.
Note: The term “upper extremity” and the acronym UE will be used interchangeably throughout this document.
Results Table
View results table
Outcomes
Acute phase - NeReBot
One high quality RCT (Masiero et al., 2011) investigated the effects of UE robot-assisted training using the NeReBot on dexterity among patients with acute stroke. This high quality RCT randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot system or conventional rehabilitation. Robot-assisted training consisted of assisted paretic elbow and shoulder movements simulating a hand-over-hand therapy. There were no significant between-group differences in dexterity (Box and Block Test) at post-treatment (5 weeks) or follow-up (3 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using NeReBot is not more effective than conventional care for improving dexterity in patients with acute stroke.
Functional independence
Effective
1a
Three high quality RCTs (Masiero et al, 2007; Rosati et al., 2007; Masiero et al., 2011) investigated the effects of UE robot-assisted training using the NeReBot on functional independence among patients with acute stroke.
The first high quality RCT (Masiero et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or a control intervention in which patients used the NeReBot with their less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There were significant between-group differences in patients’ functional independence (Functional Independence Measure total and motor scores) at post-treatment (5 weeks) and follow-up (3 and 8 months post-stroke), in favour of NeReBot training compared to the control intervention.
The second high quality RCT (Rosati et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or a control intervention in which patients used the NeReBot with their less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There were significant between-group differences in patients’ functional independence (Functional Independence Measure total and motor scores) at 3 months post-stroke, in favour of NeReBot training compared to the control intervention.
The third high quality RCT (Masiero et al., 2011) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot system or conventional rehabilitation. Robot-assisted training consisted of assisted paretic elbow and shoulder movements simulating a hand-over-hand therapy. There were no significant between-group differences in patients’ functional independence (Functional Independence Measure motor subscale) at post-treatment (5 weeks) or follow-up (3 months).
Conclusion: There is strong evidence (level 1a) from two high quality RCTs that UE training using NeReBot is more effective than comparison interventions (limited exposure to the robotic device using the less affected arm) for improving functional independence in patients with acute stroke.
Note: However, a third high quality RCT found no significant difference between UE robot-assisted training and conventional rehabilitation.
One high quality RCT (Rosati et al., 2007) investigated the effects of UE robot-assisted training using the NeReBot on pain among patients with acute stroke. This high quality RCT randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There was no significant between-group difference in UE pain (Visual Analogue Scale) at 3 months post-stroke.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using NeReBot is not more effective than a comparison intervention (limited exposure to the device using the less-affected arm) in managing UE pain in patients with acute stroke.
Spasticity
Not Effective
1A
Two high quality RCTs (Masiero et al., 2007; Masiero et al., 2011) investigated the effects of UE robot-assisted training using the NeReBot on UE spasticity among patients with acute stroke
The first high quality RCT (Masiero et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There were no significant between-group differences in UE spasticity (Modified Ashworth Scale) at post-treatment (5 weeks) or follow-up (3 and 8 months post-stroke).
The second high quality RCT (Masiero et al., 2011) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or conventional rehabilitation. Robot-assisted training consisted of assistive paretic elbow and shoulder movements simulating a hand-over-hand therapy. There was no significant between-group difference in UE spasticity (Modified Ashworth Scale) at post-treatment (5 weeks) or follow-up (3 months).
Conclusion: There is strong evidence (level 1a) from two high quality RCTs that UE training using NeReBot is not more effective than comparison interventions (conventional rehabilitation, limited exposure to the robotic device using the less affected arm) in managing UE spasticity in patients with acute stroke.
Three high quality RCTs (Masiero et al., 2007; Rosati et al., 2007; Masiero et al., 2011) investigated the effects of UE robot-assisted training using the NeReBot on UE muscle strength among patients with acute stroke.
The first high quality RCT (Masiero et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There was a significant between-group difference in deltoid strength (Medical Research Council – MRC scale of motor power) at post-treatment (5 weeks) and both follow-up (3 and 8 months post-stroke), and in biceps strength (MRC test of motor power) at post-treatment (5 weeks) and follow-up (3 months only), in favour of robot-assisted training compared to limited exposure to the device.
Note: There were no significant between-group differences in MRC wrist flexor scores at any time point.
The second high quality RCT (Rosati et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There was a significant between-group difference in UE muscle strength (MRC scale of motor power) on shoulder flexion/abduction and elbow flexion/extension at 3 months post-stroke, in favour of robot-assisted training compared to limited exposure to the device.
Note: there were no significant between-group differences in MRC wrist flexion/extension scores at 3 months post-stroke.
The third high quality RCT (Masiero et al., 2011) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot system or conventional rehabilitation. Robot-assisted training consisted of assisted paretic elbow and shoulder movements simulating a hand-over-hand therapy. There were no significant between-group differences in most measures of UE muscle strength (MRC scale of motor power, scores for deltoid, biceps, triceps, wrist extensors) at post-treatment (5 weeks) or follow-up (3 months).
Note: However, there was a significant between-group difference in MRC wrist flexor scores at post-treatment (5 weeks) only, in favour of conventional rehabilitation compared to UE robot-assisted training.
Conclusion: There is strong evidence (level 1a) from two high quality RCTs that UE training using NeReBot is more effective than comparison interventions (limited exposure to the robotic device using the less affected arm) for improving shoulder and elbow strength in patients with acute stroke.
Note: However, a third high quality RCT found no significant difference between UE robot-assisted training and conventional rehabilitation.
Trunk Control
Not Effective
1b
One high quality RCT (Masiero et al., 2007) investigated the effects of UE robot-assisted training using the NeReBot on trunk control among patients with acute stroke. This high quality RCT randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There were no significant between-group differences in trunk control (Trunk Control Test) at post-treatment (5 weeks) or follow-up (3 and 8 months post-stroke).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using NeReBot is not more effective than a comparison intervention (limited exposure to the device using the less-affected arm) for improving trunk control in patients with acute stroke.
Three high quality RCTs (Masiero et al, 2007; Rosati et al., 2007; Masiero et al., 2011) investigated the effects of UE robot-assisted training using the NeReBot on UE function among patients with acute stroke.
The first high quality RCT (Masiero et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There was a significant between-group difference in UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow + coordination score) at post-treatment (5 weeks) and follow-up (3 and 8 months post-stroke), in favour of UE robot-assisted training compared to limited exposure to the robotic device.
Note: However, there was no significant between-group difference in Fugl-Meyer Assessment of Upper Extremity wrist/hand scores at any time point.
The second high quality RCT (Rosati et al., 2007) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot or limited exposure to the device using the less affected arm. Robot-assisted training consisted of shoulder and elbow movement patterns exercises. There was a significant between-group difference in UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow + coordination score, Motor Status Scale shoulder/elbow score) at 3 months post-stroke, in favour of UE robot-assisted training compared to limited exposure to the robotic device.
Note: However, there were no significant between-group differences in Fugl-Meyer Assessment of Upper Extremity wrist/hand scores or Motor Status Scale wrist/hand scores at 3 months post-stroke.
The third high quality RCT (Masiero et al., 2011) randomized patients with acute stroke to receive UE robot-assisted training using the NeReBot system or conventional rehabilitation. Robot-assisted training consisted of assisted paretic elbow and shoulder movements simulating a hand-over-hand therapy. There were no significant between-group differences in UE function (Frenchay Arm Test, Fugl-Meyer Assessment of Upper Extremity Function total, shoulder/elbow + coordination and wrist/hand scores) at post-treatment (5 weeks) or follow-up (3 months).
Conclusion: There is strong evidence (level 1a) from two high quality RCTs that UE training using NeReBot is more effective than comparison interventions (limited exposure to the robotic device using the less affected UE) for improving proximal UE function (but not distal function) in patients with acute stroke.
Note: However, a third high quality RCT found no significant difference in UE function between NeReBot training and conventional rehabilitation.
Acute phase - MIT-Manus
Functional independence
Conflicting
4
Two high quality RCTs (Volpe et al., 2000 and Rabadi et al., 2008) and one quasi-experimental study (Aisen et al., 1997 and Volpe et al., 1999 follow up study) investigated the effects of UE robot-assisted training using the MIT-Manus on functional independence among patients with acute stroke.
The first high quality RCT (Volpe et al., 2000) randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus or limited exposure to a robotic device. Robot-assisted training consisted of goal-directed, active-assisted and passive paretic shoulder and elbow movements. There was a significant between-group difference in patients’ functional independence (FIM motor and cognition scores) at post-treatment (6-7 weeks), in favour of UE robot-assisted training.
The second high quality RCT (Rabadi et al., 2008) randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus, UE training using the Monark arm ergometer (bidirectional hand cycle) or group occupational therapy. Robot-assisted training comprised goal-directed, active-assisted and passive paretic shoulder and elbow movements. There was no significant between-group difference in patients’ functional independence (Functional Independence Measure (FIM) total, motor and cognition scores) at post-treatment (12 sessions).
A quasi-experimental study (Aisen et al., 1997) allocated patients with acute stroke to receive UE robot-assisted training using the MIT-Manus or sham robot-assisted UE training. Robot-assisted training comprised goal-directed paretic elbow and shoulder movements. There was no significant between-group difference in patients’ functional independence (FIM) at discharge (9 weeks).
In a follow-up to the study by Aisen et al., (1997) (Volpe et al., 1999) there was no significant between-group difference in patients’ functional independence (FIM) at 3 years post-stroke.
Conclusion: There is conflicting evidence (level 4) regarding the effectiveness of UE robot-assisted training using the MIT-Manus device for improving functional independence in patients with acute stroke. While onehigh quality RCTfound robot-assisted UE training to be more effective than limited exposure to the device, a second high quality RCT and a quasi-experimental study found that robot-assisted UE training using the MIT-Manus was no more effective than comparison interventions (UE ergometry, group occupational therapy, sham robot training).
One high quality RCT (Rabadi et al., 2008) investigated the effects of UE robot-assisted training using the MIT-Manus on UE pain among patients with acute stroke. This high quality RCT randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus, UE training using the Monark arm ergometer (bidirectional hand cycle) or group occupational therapy. Robot-assisted training consisted of goal-directed, active-assisted and passive paretic arm movements. There was no significant between-group difference in patients’ UE pain (Fugl-Meyer Assessment of the Upper Extremity pain score) at post-treatment (12 sessions).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using MIT-Manus is not more effective than comparison interventions (UE ergometry, group occupational therapy) in the management of UE pain in patients with acute stroke.
Spasticity
Not effective
1b
One high quality RCT (Rabadi et al., 2008) investigated the effects of UE robot-assisted training using the MIT-Manus on UE spasticity among patients with acute stroke. This high quality RCT randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus, UE training using the Monark arm ergometer (bidirectional hand cycle) or group occupational therapy. Robot-assisted training consisted of goal-directed, active-assisted and passive paretic arm movements. There was no significant between-group difference in patients’ UE spasticity (Modified Ashworth Scale) at post-treatment (12 sessions).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using MIT-Manus is not more effective than comparison interventions (UE ergometry, group occupational therapy) in the management of UE spasticity in patients with acute stroke.
Two high quality RCTs (Volpe et al., 2000 and Fasoli et al., 2004 retrospective study; Rabadi et al., 2008) and one quasi-experimental study (Aisen et al., 1997 and Volpe et al., 1999 follow-up study) investigated the effects of UE robot-assisted training using the MIT-Manus on UE strength among patients with acute stroke.
The first high quality RCT (Volpe et al., 2000) randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus or limited exposure to a robotic device. Robot-assisted therapy consisted of goal-directed, active-assisted and passive paretic shoulder and elbow movements. There was a significant between-group difference in patients’ UE strength (MRC scale of motor power) at post-treatment (6-7 weeks), in favour of UE robot-assisted training compared to limited exposure to a robotic device.
Further, a retrospective analysis of the study by Volpe et al. (2000) (Fasoli et al., 2004) found significant between-group differences in patients’ UE strength (MRC scale of motor power) from interim to discharge, in favour of UE robot-assisted training.
The second high quality RCT (Rabadi et al., 2008) randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus, UE training using the Monark arm ergometer (bidirectional hand cycle) or group occupational therapy. Robot-assisted training consisted of goal-directed, active-assisted and passive paretic shoulder and elbow movements. There was no significant between-group difference in patients’ UE strength (MRC scale of motor power) at post-treatment (12 sessions).
A quasi-experimental study (Aisen et al., 1997) allocated patients with acute stroke to receive UE robot-assisted training using the MIT-Manus or sham robot-assisted UE training. Robot-assisted training consisted of goal-directed paretic elbow and shoulder movements. There was no significant between-group difference in patients’ UE strength (motor power score measured using a 5-point scale) at discharge (9 weeks).
Further, in a follow-up to the study by Aisen et al. (1997) (Volpe et al., 1999) there was no significant between-group difference in patient’s UE strength (motor power score measured using a 5-point scale) at 3 years post-stroke.
Conclusion: There is conflicting evidence (level 4) regarding the effectiveness of UE robot-assisted training using the MIT-Manus device for improving UE strength in patients with acute stroke. While one high quality RCT found robot-assisted UE training to be more effective than limited exposure to the device, a second high quality RCT and a quasi-experimental study found that robot-assisted UE training using the MIT-Manus was no more effective than comparison interventions (UE ergometry, group occupational therapy, sham robot training).
UE Function
Not effective
1a
Two high quality RCTs (Volpe et al., 2000 and Fasoli et al., 2004 retrospective study; Rabadi et al., 2008) and one quasi-experimental study (Aisen et al., 1997 and Volpe et al., 1999 follow up study) investigated the effects of UE robot-assisted training using the MIT-Manus on UE function among patients with acute stroke.
The first high quality RCT (Volpe et al., 2000) randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus or limited exposure to a robotic device. Robot-assisted training consisted of goal-directed, active-assisted and passive paretic shoulder and elbow movements. There was no significant between-group difference in most measures of patients’ UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow and wrist/hand scores, Motor Status Scale wrist/hand scores) at post-treatment (7 weeks).
Note: However, there was a significant difference in patients’ Motor Status Scale shoulder/elbow and coordination score, in favour of UE robot-assisted training compared to limited exposure to a robotic device.
A retrospective analysis of the study by Volpe et al., (2000) (Fasoli et al., 2004) reported significant group by time interactions in patients’ UE functional (Fugl-Meyer Assessment of Upper Extremity, Motor Status Scale shoulder/elbow score) from interim to discharge evaluations, in favour of robot-assisted training compared to limited exposure to the robotic device.
Note: There were no significant between-group differences in patients’ Motor Status Scale wrist/hand scores from interim to discharge.
The second high quality RCT (Rabadi et al., 2008) randomized patients with acute stroke to receive UE robot-assisted training using the MIT-Manus, UE training using the Monark arm ergometer (bidirectional hand cycle), or group occupational therapy. Robot-assisted therapy consisted of goal-directed, active-assisted and passive paretic shoulder and elbow movements. There were no significant between-group differences in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow and wrist/hand scores, Motor Status Scale shoulder/elbow and wrist/hand scores, Action Research Arm Test) at post-treatment (12 sessions).
A quasi-experimental study (Aisen et al., 1997) allocated patients with acute stroke to receive UE robot-assisted training using the MIT-Manus or sham robot-assisted UE training. Robot-assisted training consisted of goal-directed paretic elbow and shoulder movements. There was no significant between-group difference in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity, Motor Status Score proximal or distal scores) at discharge (9 weeks).
A follow-up to the study by Aisen et al. (1997) (Volpe et al., 1999) found no significant between-group differences in most measures of patients’ UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow + coordination and wrist/hand scores, Motor Status Score wrist/hand score) at 3 years post-stroke.
Note: There was a significant between-group difference in patients’ Motor Status Scale shoulder/elbow scores, in favour of UE robot-assisted training compared to the sham intervention.
Conclusion: There is strong evidence (level 1a) from two high quality RCTs that UE training using MIT-Manus is not more effective than comparison interventions (UE ergometry, group occupational therapy, sham robot-assisted UE training) for improving UE function in patients with acute stroke.
Subacute phase - MIME
Functional Independence
Not Effective
2A
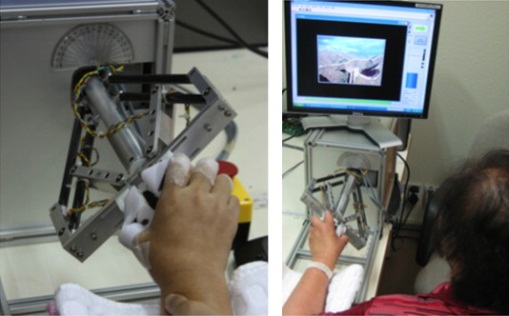
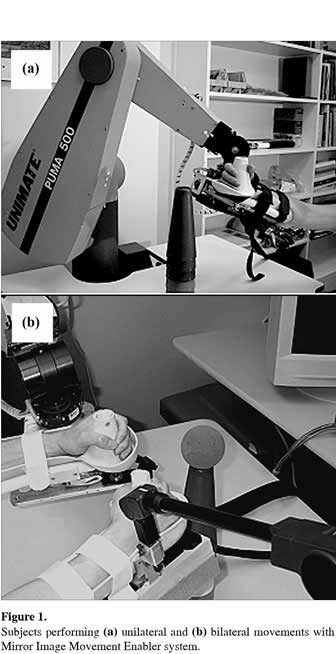
MIME (Mirror Image Movement Enabler)
One fair quality RCT (Lum et al., 2006) investigated the effects of UE robot-assisted training using the MIME device on functional independence among patients with subacute stroke. This fair quality RCT randomized patients with subacute stroke to receive unilateral, bilateral or combined unilateral and bilateral UE robot-assisted training using the MIME robot, or conventional rehabilitation. Robot-assisted training comprised goal-directed paretic elbow and shoulder reaching movements. There were no significant differences in functional independence (Functional Independence Measure (FIM) self-care and transfers scores) among groups at post-treatment (4 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that unilateral and/or bilateral UE training using the MIME device is not more effective than conventional rehabilitation for improving functional independence in patients with subacute stroke.
Spasticity
Not Effective
2A
MIME (Mirror Image Movement Enabler)
One fair quality RCT (Lum et al., 2006) investigated the effects of UE robot-assisted training using the MIME device on UE spasticity among patients with subacute stroke. This fair quality RCT randomized patients with subacute stroke to receive unilateral, bilateral or combined unilateral and bilateral UE robot-assisted training using the MIME robot, or conventional rehabilitation. Robot-assisted training consisted of goal-directed paretic elbow and shoulder reaching movements. There were no significant between-group differences in UE spasticity (Modified Ashworth Scale proximal and distal scores) among groups at post-treatment (4 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that unilateral and/or bilateral UE training using MIME device is not more effective than conventional rehabilitation for managing UE spasticity in patients with subacute stroke.
MIME (Mirror Image Movement Enabler)
One fair quality RCT (Lum et al., 2006) investigated the effects of UE robot-assisted training using the MIME device on UE strength among patients with subacute stroke. This fair quality RCT randomized patients with subacute stroke to receive unilateral, bilateral or combined unilateral and bilateral UE robot-assisted training using the MIME robot, or conventional rehabilitation. Robot-assisted training consisted of goal-directed paretic elbow and shoulder reaching movements. There were no significant between-group differences in UE strength (motor power measured using a 5-point scale) among groups at post-treatment (4 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that unilateral and/or bilateral UE training using the MIME device is not more effective than conventional rehabilitation for improving UE strength in patients with subacute stroke.
MIME (Mirror Image Movement Enabler)
One fair quality RCT (Lum et al., 2006) investigated the effects of UE robot-assisted training using the MIME device on UE function among patients with subacute stroke. This fair quality RCT randomized patients with subacute stroke to receive unilateral and/or bilateral UE robot-assisted training using the MIME robot, or conventional rehabilitation. Robot-assisted training consisted of goal-directed paretic elbow and shoulder reaching movements. At post-treatment (4 weeks) there were significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow score, Motor Status Scale synergy score), favoring combined unilateral+bilateral robot-assisted training compared to conventional rehabilitation. There were no significant differences in Fugl-Meyer Assessment of Upper Extremity wrist/hand scores among groups at post-treatment. At follow-up (6 months) there was a significant between-group difference in UE function (Fugl-Meyer Assessment of Upper Extremity wrist/hand score) in favour of unilateral robot-assisted training compared to combined unilateral+bilateral robot-assisted training. There were no significant between-group differences in other measures of UE function (Fugl-Meyer Assessment of Upper Extremity shoulder/elbow score, Motor Status Scale synergy score) at follow-up.
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using the MIME device is more effective than conventional care for improving UE function in patients with subacute stroke.
Note: Differences were only significant between combined unilateral+bilateral robot-assisted training vs. conventional rehabilitation at post-treatment.
Chronic phase - Active Joint Brace for the Elbow
One quasi-experimental study (Stein et al., 2007) investigated the effects of UE robot-assisted training using an active elbow brace on UE spasticity among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using an EMG-controlled exoskeletal robotic brace. Robot-assisted training comprised UE functional tasks performed using the elbow brace. There was a significant improvement in UE spasticity (Modified Ashworth Scale) at post-treatment (6-9 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using an EMG-controlled exoskeletal robotic brace is effective in managing UE spasticity in patients with chronic stroke.
One quasi-experimental study (Stein et al., 2007) investigated the effects of UE robot-assisted training using an active elbow brace on UE function among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using an EMG-controlled exoskeletal robotic brace. Robotic training comprised UE functional tasks performed using the elbow brace. There was a significant improvement in UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (6-9 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental studythat UE training using an EMG-controlled exoskeletal robotic brace is effective for improving UE function in patients with chronic stroke.
Chronic phase - ARMGuide
Kinematics
Not Effective
1B
One high quality RCT (Kahn et al., 2001) and one fair quality RCT (Kahn et al., 2006) investigated the effects of UE robot-assisted training using the ARM Guide system on UE kinematics among patients with chronic stroke.
The high quality RCT (Kahn et al., 2001) randomized patients with chronic stroke to receive robot-assisted upper extremity training using the ARM Guide or task-matched non-robotic free-reaching training. Robot-assisted training consisted of assisted goal-directed forward reaching movements to a set of 7 targets. There were no significant between-group differences in UE kinematics (peak velocity during reaching, passive resistance to movement) at post-treatment (8 weeks).
The fair quality RCT (Kahn et al., 2006) randomized patients with chronic stroke to receive UE robot-assisted training using the ARM Guide or task-matched non-robotic free-reaching training. Robot-assisted training consisted of active-assisted reaching exercises to 5 targets. There were no significant between-group differences in most UE kinematic measures (limb stiffness, active supported reach range, free-reach unsupported range, reach velocity, free-reach straightness) at post-treatment (8 weeks).
Note: however, there was a significant between-group difference in free-reach smoothness at post-treatment, in favour of robot-assisted training compared to free-reaching exercises.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCT that UE training using ARM Guide system is not more effective than comparison interventions (task-matched non-robotic free-reach training) for improving UE kinematics in patients with chronic stroke.
Range of motion
Not Effective
1B
One high quality RCT (Kahn et al., 2001) investigated the effects of UE robot-assisted training using the ARM Guide on UE range of motion (ROM) among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive robot-assisted upper extremity training using the ARM Guide or task-matched non-robotic free-reaching training. Robot-assisted training consisted of assisted goal-directed forward reaching movements to a set of 7 targets. There were no significant between-group differences in UE active range of motion at post-treatment (8 weeks).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE robot-assisted training using the ARM Guide is not more effective than a comparison intervention (task-matched non-robotic training) for improving range of motion in patients with chronic stroke.
UE function
Not Effective
1B
One high quality RCT (Kahn et al., 2001) and one fair quality RCT (Kahn et al., 2006) investigated the effects of UE robot-assisted training using the ARM Guide system on UE function among patients with chronic stroke.
The high quality RCT (Kahn et al., 2001) randomized patients with chronic stroke to receive robot-assisted upper extremity training or task-matched non-robotic free-reaching training. Robot-assisted upper extremity training consisted of assistive goal-directed forward reaching movements to a set of 7 targets. There was no significant between-group difference in UE function (Chedoke McMaster Scale, Rancho Los Amigos Test for the Hemiparetic Upper Extremity) at post-treatment (8 weeks).
The fair quality RCT (Kahn et al., 2006) randomized patients with chronic stroke to received UE robot-assisted training using the ARM Guide device or task-matched non-robotic free-reaching exercises. Robot-assisted training consisted of active-assisted reaching to 5 targets at different locations. There was no significant between-group difference in UE function (Chedoke McMaster Test, Rancho Los Amigos Functional Test of the Hemiparetic Upper Extremity) at post-treatment (8 weeks).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCT that UE training using ARM Guide system is not more effective than comparison interventions (task-matched non-robotic free-reach training) for improving UE function in patients with chronic stroke.
Chronic phase - ARMin I / II
One single-case study (Nef et al., 2009) investigated the effects of UE robot-assisted training using the ARMin I system on UE coordination among patients with chronic stroke. This single-case study provided 3 patients with chronic stroke with UE robot-assisted training using the ARMin I device. Robot-assisted training comprised goal-directed forearm and shoulder reaching movements with haptic visual and sound feedback. Patients demonstrated a significant improvement in UE coordination on transversal abduction/adduction and elbow flexion at 8 weeks (post-treatment). Improvements in coordination did not remain significant at follow-up (16 weeks).
Conclusion: There is limited evidence (level 2b) from one single-case study that UE training using ARMin I system is effective for improving UE coordination in patients with chronic stroke in the short-term.
Functional Independence
Not Effective
2B
One single-case study (Nef et al., 2009) investigated the effects of UE robot-assisted training using the ARMin I system on functional independence among patients with chronic stroke. This single-case study provided 3 patients with chronic stroke with UE robot-assisted training using the ARMin I device. Robot-assisted training comprised goal-directed forearm and shoulder reaching movements with haptic visual and sound feedback. There was no significant improvement in patients’ functional independence (Barthel Index) at post-treatment (8 weeks) or follow-up (16 weeks).
Conclusion: There is limited evidence (level 2b) from one single-case study that UE training using ARMin I system is not effective for improving functional independence in patients with chronic stroke.
Kinematics
Not Effective
2B
One single-case study (Staubli et al., 2009) investigated the effects of UE robot-assisted training using the ARMin II system on UE kinematics among patients with chronic stroke. This single-case study provided 4 patients with chronic stroke with robot-assisted upper extremity training using the ARMin II exoskeleton robot (6 degrees of freedom moving shoulder, elbow and wrist joints). Robot-assisted training included passive-assisted and active-assisted goal-directed exercises with visual and auditory feedback. There was no significant improvement in UE kinematics (maximal voluntary torques) at post-treatment (8 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2b) from one single-case study indicate that the ARMin II system is not effective for improving UE kinematics in patients with chronic stroke.
Range of Motion
Effective
2B
One single-case study (Nef et al., 2009) investigated the effects of UE robot-assisted training using the ARMin I system on UE range of motion (ROM) among patients with chronic stroke. This single-case study provided 3 patients with chronic stroke with UE robot-assisted training using the ARMin I device. Robot-assisted training consisted of goal-directed forearm and shoulder reaching movements with haptic visual and sound feedback. There was a significant improvement for 2 of 3 patients in elbow active range of motion (flexion/extension) at post-treatment (8 weeks) and follow-up (16 weeks). However, there were no significant improvements in shoulder active range of motion (shoulder abduction, transversal abduction, shoulder flexion) at post-treatment or follow-up.
Conclusion: There is limited evidence (level 2b) from one single-case study that UE training using ARMin I system is effective for improving range of motion at the elbow (but not the shoulder) in patients with chronic stroke.
Satisfaction
Not Effective
2B
One single-case study (Staubli et al., 2009) investigated the effects of UE robot-assisted training using the ARMin II system on satisfaction among patients with chronic stroke. This single-case study provided 4 patients with chronic stroke with robot-assisted upper extremity training using the ARMin II exoskeleton robot (6 degrees of freedom moving shoulder, elbow and wrist joints). Robot-assisted training comprised passive-assisted and active-assisted goal-directed exercises with visual and auditory feedback. There were no significant improvements in patients’ satisfaction (subjective assessment of ADL tasks, progress, changes and motivation using a non-standardized questionnaire) at post-treatment (8 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2b) from one single-case study show that the ARMin II system is not effective for improving satisfaction among patients with chronic stroke.
One single-case study (Staubli et al., 2009) investigated the effects of UE robot-assisted training using the ARMin II system on UE sensation among patients with chronic stroke. This single-case study provided 4 patients with chronic stroke with robot-assisted upper extremity training using the ARMin II exoskeleton robot (6 degrees of freedom moving shoulder, elbow and wrist joints). Robot-assisted training comprised passive-assisted and active-assisted goal-directed exercises with visual and auditory feedback. There were no significant improvements in patients’ UE sensation (American Spinal Cord Injury Association Test) at post-treatment (8 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2b) from one single-case study show that the ARMin II system is not effective for improving UE sensation in patients with chronic stroke.
One single-case study (Nef et al., 2009) investigated the effects of UE robot-assisted training using the ARMin I system on UE strength among patients with chronic stroke. This single-case study provided 3 patients with chronic stroke with UE robot-assisted training using the ARMin I device. Robot-assisted training comprised goal-directed forearm and shoulder reaching movements with haptic visual and sound feedback. There was a significant improvement in patients’ UE strength (shoulder extension/adduction, shoulder flexion/abduction and transverse abduction) at post-treatment (8 weeks) and follow-up (16 weeks after treatment).
Note: There were no significant improvements in UE strength on shoulder transverse adduction at either time point.
Conclusion: There is limited evidence (level 2b) from one single-case study that UE training using ARMin I system is effective for improving shoulder strength in patients with chronic stroke.
Two single-case studies (Nef et al., 2009 and Staubli et al., 2009) investigated the effects of UE robot-assisted training using the ARMin I or II systems on UE function among patients with chronic stroke.
The first single-case study (Nef et al., 2009) provided 3 patients with chronic stroke with UE robot-assisted training using the ARMin I device. Robot-assisted training comprised goal-directed forearm and shoulder reaching movements with haptic visual and sound feedback. All three participants showed a significant improvement in UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (8 weeks), and results remained significant for one of three participants at follow-up (16 weeks).
Note: There were no significant improvements in another measure of UE function (Action Research Arm Test) at post-treatment or follow-up.
The second single-case study (Staubli et al., 2009) provided 4 patients with chronic stroke with robot-assisted upper extremity training using the ARMin II exoskeleton robot (6 degrees of freedom moving shoulder, elbow and wrist joints). Robot-assisted training included passive-assisted and active-assisted goal-directed exercises with visual and auditory feedback. There was a significant improvement in UE function (Fugl-Meyer Assessment of Upper Extremity Function, Wolf Motor Function Test) among three of four participants at post-treatment (8 weeks) and follow-up (6 months).
Conclusion: There is limited evidence (level 2b) from two single-case design studies that UE training using the ARMin I and ARMin II systems is effective for improving UE function in patients with chronic stroke.
Unilateral neglect
Not Effective
2B
One single-case design study (Staubli et al., 2009) investigated the effects of UE robot-assisted training using the ARMin I or II systems on unilateral neglect among patients with chronic stroke. This single-case study provided 4 patients with chronic stroke with robot-assisted upper extremity training using the ARMin II exoskeleton robot (6 degrees of freedom moving shoulder, elbow and wrist joints). Robot-assisted training included passive-assisted and active-assisted goal-directed exercises with visual and auditory feedback. There were no significant improvements in unilateral neglect (Catherine Bergego Scale) at post-treatment (8 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2b) from a single-case design study indicate that the ARMin II device is not effective for improving unilateral neglect in patients with chronic stroke.
Chronic phase - BATRAC
Grip strength
Not Effective
2B
BATRAC (Bilateral Arm Training with Rhythmic Auditory Cueing)
One quasi-experimental study (Whitall et al., 2000) investigated the effects of UE robot-assisted training using the BATRAC system on grip strength among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BATRAC device. Robot-assisted training consisted of bilateral arm training with rhythmic auditory cueing to push and pull two sliding bar handles in the transverse plane. There was no significant improvement in grip strength (measured by BASELINE Hydraulic Hand Dynamometer) at post-treatment (6 weeks) or follow-up (2 months).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BATRAC system is not effective for improving grip strength in patients with chronic stroke.
Range of motion
Effective
2b
BATRAC (Bilateral Arm Training with Rhythmic Auditory Cueing)
One quasi-experimental study (Whitall et al., 2000) investigated the effects of UE robot-assisted training using the BATRAC system on range of motion (ROM) among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BATRAC device. Robot-assisted training consisted of bilateral arm training with rhythmic auditory cueing to push and pull two sliding bar handles in the transverse plane. At post-treatment (6 weeks) there were significant improvements in some measures of range of motion (measured using a goniometer) of the paretic shoulder (active ROM on extension), wrist (active and passive ROM on flexion) and thumb (active ROM on opposition). At follow-up (2 months) improvements remained significant for active ROM on thumb opposition of the paretic limb only.
Note: there were no significant improvements in active or passive elbow ROM at either time point.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BATRAC system is effective for improving range of motion on some shoulder, wrist and thumb movements in patients with chronic stroke.
BATRAC (Bilateral Arm Training with Rhythmic Auditory Cueing)
One high quality RCT (Luft et al., 2004) and one quasi-experimental study (Whitall et al., 2000) investigated the effects of UE robot-assisted training using the BATRAC system on UE strength among patients with chronic stroke.
The high quality RCT (Luft et al., 2004) randomized patients with chronic stroke to receive UE robot-assisted training using the BATRAC device or standardized dose-matched therapeutic exercises. Robot-assisted training consisted of 6 weeks of bilateral arm training with rhythmic auditory cueing to push and pull two sliding bar handles in the transverse plane. There was no significant between-group difference in patients’ elbow and shoulder strength (measures using dynamometry) at 2 weeks post-intervention (8 weeks).
The quasi-experimental study (Whitall et al., 2000) provided patients with chronic stroke with UE robot-assisted training using the BATRAC device. Robot-assisted training consisted of bilateral arm training with rhythmic auditory cueing to push and pull two sliding bar handles in the transverse plane. At post-treatment (6 weeks) there was a significant improvement in elbow isometric strength and wrist flexion isometric strength (paretic UE only), but no significant improvement in shoulder or thumb opposition isometric strength. At follow-up (2 months) results were significant for elbow flexion and wrist extension isometric strength (non-paretic UE only); changes in shoulder isometric strength remained insignificant at follow-up.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the BATRAC system is not more effective than a comparison intervention (dose-matched therapeutic exercises) for improving UE strength in patients with chronic stroke. However, a quasi-experimental study reported improvements in elbow and wrist strength following BATRAC training.
UE function
Not Effective
1B
BATRAC (Bilateral Arm Training with Rhythmic Auditory Cueing)
One high quality RCT (Luft et al., 2004) and one quasi-experimental study (Whitall et al., 2000) investigated the effects of UE robot-assisted training using the BATRAC system on UE function among patients with chronic stroke
The high quality RCT (Luft et al., 2004) randomized patients with chronic stroke to receive UE robot-assisted training using the BATRAC device or standardized dose-matched therapeutic exercises. Robot-assisted training consisted of bilateral arm training of 6 weeks with rhythmic auditory cueing to push and pull two sliding bar handles in the transverse plane. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity Function, Wolf Motor Function Test weight and time scores) or daily use of the hemiparetic arm (University of Maryland Arm Questionnaire for Stroke) at 2 weeks post-intervention (8 weeks).
Note: However, there was a significant between-group difference in Fugl-Meyer Assessment of Upper Extremity Function scores in a subgroup analysis of patients with a positive Functional magnetic resonance imaging (fMRI) response at 2 weeks post-intervention, in favour of BATRAC compared to standardized dose-matched therapeutic exercises.
The quasi-experimental study (Whitall et al., 2000) provided patients with chronic stroke with UE robot-assisted training using the BATRAC device. Robot-assisted training consisted of bilateral arm training with rhythmic auditory cueing to push and pull two sliding bar handles in the transverse plane. There were significant improvements in UE function (Fugl-Meyer Assessment of Upper Extremity Function, Wolf Motor Function Test performance time score) and daily use of the hemiparetic arm (University of Maryland Arm Questionnaire for Stroke) at post-treatment (6 weeks) and follow-up (2 months).
Note: There were no significant improvements in Wolf Motor Function Test strength or function scores at either time point.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the BATRAC system is not more effective than a comparison intervention (dose-matched therapeutic exercises) for improving UE function in patients with chronic stroke. However, a quasi-experimental study reported improvements in UE function following BATRAC training.
Chronic phase - Bilateral Forearm and Wrist Trainer
Satisfaction
Not Effective
2B
One quasi-experimental study (Hesse et al., 2003) investigated the effects of UE robot-assisted training using the Bilateral Forearm and Wrist Trainer system on satisfaction among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with robot-assisted upper extremity training using a portable, 1 degree-of-freedom trainer device that allowed for bilateral passive and active practice of 2 movements: elbow pronation/supination and wrist dorsiflexion/volarflexion. There was no significant change in patients’ satisfaction regarding the effect of treatment on muscle tone, motor control and competence in activities of daily living (measured using a standardized questionnaire) at post-treatment (3 weeks) or follow-up (3 months).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the Bilateral Forearm and Wrist Trainer system is not effective for improving satisfaction of patients with chronic stroke.
One quasi-experimental study (Hesse et al., 2003) investigated the effects of UE robot-assisted training using the Bilateral Forearm and Wrist Trainer system on UE spasticity among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with robot-assisted upper extremity training using a portable, 1 degree-of-freedom trainer device that allowed for bilateral passive and active practice of 2 movements: elbow pronation/supination and wrist dorsiflexion/volarflexion. There was a significant improvement in patients’ wrist/finger spasticity (Modified Ashworth Scale) at post-treatment (3 weeks) but results did not remain significant at follow-up (3 months). There was no significant change in patients’ elbow spasticity (Modified Ashworth Scale) at either time point.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the Bilateral Forearm and Wrist Trainer system is effective in managing wrist/finger spasticity in patients with chronic stroke in the short term. There was no significant effect of treatment on elbow spasticity.
UE function
Not Effective
2B
One quasi-experimental study (Hesse et al., 2003) investigated the effects of UE robot-assisted training using the Bilateral Forearm and Wrist Trainer system on UE function among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with robot-assisted upper extremity training using a portable, 1 degree-of-freedom trainer device that allowed for bilateral passive and active practice of 2 movements: elbow pronation/supination and wrist dorsiflexion/volarflexion. There was no significant change in patients’ UE function (Rivermead Motor Assessment) at post-treatment (3 weeks) or follow-up (3 months).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the Bilateral Forearm and Wrist Trainer system is not effective for improving UE function in patients with chronic stroke.
Chronic phase - BFIAMT
BFIAMT (Bilateral force-induced isokinetic arm movement training)
One quasi-experimental study (Chang et al., 2007) investigated the effects of UE robot-assisted training using the BFIAMT system on grip strength among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BFIAMT system. Robot-assisted training consisted of bilateral force-induced arm movements. There was a significant improvement in patients’ grip strength at post-treatment (8 weeks) and follow-up (16 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BFIAMT system is effective for improving grip strength in patients with chronic stroke.
BFIAMT (Bilateral force-induced isokinetic arm movement training)
One quasi-experimental study (Chang et al., 2007) investigated the effects of UE robot-assisted training using the BFIAMT system on kinematic outcomes among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BFIAMT system. Robot-assisted training consisted of bilateral force-induced arm movements. There was a significant improvement in kinematic outcomes (peak velocity, percentage of time to peak velocity, movement time, normalized jerk) at post-treatment (8 weeks) but results did not remain significant at post-treatment (16 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BFIAMT system is effective for improving kinematic outcomes in patients with chronic stroke in the short term.
Spasticity
Not Effective
2B
BFIAMT (Bilateral force-induced isokinetic arm movement training)
One quasi-experimental study (Chang et al., 2007) investigated the effects of UE robot-assisted training using the BFIAMT system on UE spasticity among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BFIAMT system. Robot-assisted training consisted of bilateral force-induced arm movements. There was no significant improvement in patients’ UE spasticity (Modified Ashworth Scale) at post-treatment (8 weeks) or follow-up (16 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BFIAMT system is not effective in managing UE spasticity in patients with chronic stroke.
BFIAMT (Bilateral force-induced isokinetic arm movement training)
One quasi-experimental study (Chang et al., 2007) investigated the effects of UE robot-assisted training using the BFIAMT system on UE strength among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BFIAMT system. Robot-assisted training consisted of bilateral force-induced arm movements. There was a significant improvement in patients’ UE push and pull strength at post-treatment (8 weeks) and follow-up (16 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BFIAMT system is effective for improving UE strength in patients with chronic stroke.
BFIAMT (Bilateral force-induced isokinetic arm movement training)
One quasi-experimental study (Chang et al., 2007) investigated the effects of UE robot-assisted training using the BFIAMT system on UE function among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the BFIAMT system. Robot-assisted training consisted of bilateral force-induced arm movements. There was a significant improvement in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (8 weeks) and follow-up (16 weeks).
Note: However, there was no significant improvement in patients’ Frenchay Arm Test scores at post-treatment or follow-up.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the BFIAMT system is effective for improving UE function in patients with chronic stroke.
Chronic phase - Bi-Manu-Track
Functional Independence
Not Effective
1B
One high quality RCT (Liao et al., 2011) investigated the effects of UE robot-assisted training using the Bi-Manu-Track system on functional independence among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the Bi-Manu-Track device or dose-matched conventional rehabilitation. Robot-assisted training consisted of bilateral mirror-like movement cycles of forearm pronation/supination, and wrist flexion/extension in 4 modes: passive-passive, passive-active, active-active, and active-passive. There was no significant between-group difference in functional independence (Functional Independence Measure) at post-treatment (4 weeks).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the Bi-Manu-Track system is not more effective than a comparison intervention (conventional rehabilitation) for improving functional independence in patients with chronic stroke.
One high quality RCT (Liao et al., 2011) investigated the effects of UE robot-assisted training using the Bi-Manu-Track system on UE function among patients with chronic stroke This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the Bi-Manu-Track device or dose-matched conventional rehabilitation. Robot-assisted training consisted of bilateral mirror-like movement cycles of forearm pronation/supination, and wrist flexion/extension in 4 modes: passive-passive, passive-active, active-active, and active-passive. There was a significant between-group difference in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity Function) and perceived use of the affected upper limb (ABILHAND) at post-treatment (4 weeks), in favour of robot-assisted training compared to dose-matched conventional rehabilitation.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the Bi-Manu-Track system is more effective than a comparison intervention (conventional rehabilitation) for improving UE function in patients with chronic stroke.
UE motor activity
Effective
1B
One high quality RCT (Liao et al., 2011) investigated the effects of UE robot-assisted training using the Bi-Manu-Track system on UE motor activity among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the Bi-Manu-Track device or dose-matched conventional rehabilitation. Robot-assisted training consisted of bilateral mirror-like movement cycles of forearm pronation/supination, and wrist flexion/extension in 4 modes: passive-passive, passive-active, active-active, and active-passive. There was a significant between-group difference in patients’ UE motor activity (Motor Activity Log Amount of Use and Quality of Movement scores, Arm Activity Ratio) at post-treatment (4 weeks), in favour of robot-assisted training compared to conventional rehabilitation.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the Bi-Manu-Track system is more effective than a comparison intervention (conventional rehabilitation) for improving UE function in patients with chronic stroke.
Chronic phase - Braccio di Ferro
Two quasi-experimental studies (Casadio et al., 2009; Vergaro et al., 2010) investigated the effects of UE robot-assisted training using the Braccio di Ferro system on UE kinematic outcomes among patients with chronic stroke.
The first quasi-experimental study (Casadio et al., 2009) provided patients with chronic stroke with robot-assisted upper extremity training using the Braccio di Ferro device. Robot-assisted training comprised goal-directed reaching movements from the shoulder and elbow in a horizontal plane, with visual or haptic feedback. There were significant improvements in all kinematic measures (mean speed, number of submovements, endpoint error after the first submovement, and ratio between the duration of the first submovement and the total time required for reaching the target) at post-treatment (10 weeks), but results did not remain significant at follow-up (3 months).
The second quasi-experimental study (Vergaro et al., 2010) provided patients with chronic stroke with UE robot-assisted training using the Braccio di Ferro device. Robot-assisted training consisted of 10 goal-directed continuous elbow movements following a figure-of-eight shaped trajectory. There was a significant improvement in patients’ UE kinematics (movement smoothness, movement accuracy) at end of treatment (6-12 sessions).
Conclusion: There is limited evidence (level 2b) from two quasi-experimental studies that UE training using the Braccio de Ferro system is effective for improving UE kinematics in patients with chronic stroke.
Note: For one of these studies, significant improvements were short term only.
Spasticity
Not Effective
2B
Two quasi-experimental studies (Casadio et al., 2009; Vergaro et al., 2010) investigated the effects of UE robot-assisted training using the Braccio di Ferro system on UE spasticity among patients with chronic stroke.
The first quasi-experimental study (Casadio et al., 2009) provided patients with chronic stroke with robot-assisted upper extremity training using the Braccio di Ferro device. Robot-assisted training comprised goal-directed reaching movements from the shoulder and elbow joints in a horizontal plane, with visual and haptic feedback. There was no significant change in UE spasticity of flexor muscles (Ashworth Scale) at post-treatment (10 weeks) or follow-up (3 months).
The second quasi-experimental study (Vergaro et al., 2010) provided patients with chronic strokewith UE robot-assisted training using the Braccio di Ferro device. Robot-assisted training consisted of 10 goal-directed continuous elbow movements following a figure-of-eight shaped trajectory. There was no significant change in UE spasticity (Ashworth Scale) at post-treatment (6-12 sessions).
Conclusion: There is limited evidence (level 2b) from two quasi-experimental studies that UE training using the Braccio de Ferro system is not effective in managing UE spasticity in patients with chronic stroke.
Two quasi-experimental studies (Casadio et al., 2009; Vergaro et al., 2010) investigated the effects of UE robot-assisted training using the Braccio di Ferro system on UE function among patients with chronic stroke.
The first quasi-experimental study (Casadio et al., 2009) provided patients with chronic stroke with robot-assisted upper extremity training using the Braccio di Ferro device. Robot-assisted training comprised goal-directed reaching movements from the shoulder and elbow joints in a horizontal plane, with visual and haptic feedback. There was a significant improvement in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (10 weeks), but results did not remain significant at follow-up (3 months).
The second quasi-experimental study (Vergaro et al., 2010) provided patients with chronic stroke with UE robot-assisted training using the Braccio di Ferro device. Robot-assisted training consisted of 10 goal-directed continuous elbow movements following a figure-of-eight shaped trajectory. There was a significant improvement in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (6-12 sessions).
Conclusion: There is limited evidence (level 2b) from two quasi-experimental studies that UE training using the Braccio de Ferro system is effective for improving UE function in patients with chronic stroke.
Note: For one of these studies, significant improvements were short term only.
Chronic phase - Elbow and Wrist Assistive Rehabilitation Device
Functional Independence
Not Effective
2B
One quasi-experimental study (Hu et al., 2009) investigated the effects of UE robot-assisted training using a wrist assistive rehabilitation device on functional independence among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with robot-assisted wrist training that consisted of assisted wrist flexion/extension goal-directed movements in a horizontal plane. There was no significant change in functional independence (Functional Independence Measure) from baseline to post-treatment (7 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using a wrist assistive rehabilitation device is not effective for improving functional independence in patients with chronic stroke.
Two quasi-experimental studies (Hu et al., 2007; Hu et al., 2009) investigated the effects of UE robot-assisted training using an elbow or wrist assistive rehabilitation device on UE spasticity among patients with chronic stroke.
The first quasi-experimental study (Hu et al., 2007) provided patients with chronic stroke with robot-assisted UE training that consisted of assisted elbow flexion/extension goal-directed movements in a horizontal plane. There was a significant reduction in patients’ UE spasticity (Modified Ashworth Scale) at post-treatment (7 weeks).
The second quasi-experimental study (Hu et al., 2009) provided patients with chronic stroke with robot-assisted UE training that consisted of assisted wrist flexion/extension goal-directed movements in a horizontal plane. There was a significant reduction in elbow and wrist spasticity (Modified Ashworth Scale) at post-treatment (7 weeks).
Conclusion: There is limited evidence (level 2b) from two quasi-experimental studies that UE training using an elbow or wrist assistive rehabilitation device is effective in reducing UE spasticity in patients with chronic stroke.
Two quasi-experimental studies (Hu et al., 2007; Hu et al., 2009) investigated the effects of UE robot-assisted training using an elbow or wrist assistive rehabilitation device on UE function among patients with chronic stroke.
The first quasi-experimental study (Hu et al., 2007) provided patients with chronic stroke with robot-assisted elbow training that consisted of assisted elbow flexion/extension goal-directed movements in a horizontal plane. There was a significant improvement in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity Function, Motor Status Scale) at post-treatment (7 weeks).
The second quasi-experimental study (Hu et al., 2009) provided patients with chronic stroke with robot-assisted wrist training that consisted of assisted wrist flexion/extension goal-directed movements in a horizontal plane. There was a significant improvement in UE function (Fugl-Meyer Assessment of Upper Extremity Function shoulder/elbow and wrist/hand scores) at post-treatment (7 weeks).
Note: However, there was no significant change in Action Research Arm Test scores at post-treatment.
Conclusion: There is limited evidence (level 2b) from two quasi-experimental studies that UE training using an elbow or wrist assistive rehabilitation device is effective for improving UE function in patients with chronic stroke.
Chronic phase - GENTLE/S
Range of motion
Not Effective
2B
One study of single-case series (Amirabdollahian et al., 2007) investigated the effects of UE robot-assisted training using the GENTLE/S system on UE range of motion among patients with chronic stroke. This study of 31 single-case series adopted a multiple baseline model to randomize patients with chronic stroke to receive UE robot-assisted training using the GENTLE/S system, sling suspension UE training, or no training in ABC or ACB phases (A: no training – baseline -, B: GENTLE/S system training, C: sling suspension training). GENTLE/S system training consisted of goal-directed, paretic arm reaching and withdrawal movements in 3 modes: passive, active-assisted and active. There were no reported differences in patients’ active and passive elbow/shoulder range of motion at the end of each phase (3 weeks).
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than no intervention or a comparison intervention (sling suspension UE training) for improving UE range of motion in patients with chronic stroke.
One study of single-case series (Amirabdollahian et al., 2007) investigated the effects of UE robot-assisted training using the GENTLE/S system on UE function in patients with chronic stroke. This study of 31 single-case series adopted a multiple baseline model to randomize patients with chronic stroke to receive UE robot-assisted training using the GENTLE/S system, sling suspension UE training, or no intervention in ABC or ACB phases (A: no training (baseline), B: GENTLE/S system training, C: sling suspension training). GENTLE/S system training consisted of goal-directed, paretic arm reaching and withdrawal movements in 3 modes: passive, active-assisted and active. There was a significant difference in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity) in favour of GENTLE/S system training and sling suspension UE training compared to no intervention provided at baseline. There were no significant differences in UE function between robot-assisted UE training and sling suspension UE training.
Note: There were no significant differences in Motor Assessment Scale scores between phases.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is more effective than no intervention for improving UE function in patients with chronic stroke.
Note: Robot-assisted training using the GENTLE/S system was not more effective than sling suspension UE training.
Chronic phase - HandCare
Kinematics
Insufficient evidence
5
One case study (Dovat et al., 2010) investigated the effects of UE robot-assisted training using the HandCare system on hand kinematics among patients with chronic stroke. This case study provided patients with chronic stroke with UE robot-assisted training using the HandCare device. Robot-assisted training consisted of goal-directed finger coordination and finger independence exercises using the Hand Cable-Actuated Rehabilitation (HandCARE) system. There was a significant improvement in hand kinematics (finger movement smoothness on hand opening, finger movement coordination on hand opening and closing, finger independence, force modulation of the middle finger) at post-treatment (8 weeks).
Conclusion: There is insufficient evidence (level 5) regarding the effectiveness of robot-assisted UE training using the HandCare system on hand kinematics compared to other interventions during the chronic phase of stroke recovery. However, results from one case study show that UE training using HandCare system is effective for improving hand kinematics in patients with chronic stroke.
UE function
Insufficient evidence
5
One case study (Dovat et al., 2010) investigated the effects of UE robot-assisted training using the HandCare system on UE function among patients with chronic stroke. This case study provided patients with chronic stroke with UE robot-assisted training using the HandCare device. Robot-assisted training consisted of goal-directed finger coordination and finger independence exercises using the Hand Cable-Actuated Rehabilitation (HandCARE) system. There was no significant improvement in patients’ UE function (Chedoke McMaster Impairment Inventory) at post-treatment (8 weeks).
Conclusion: There is insufficient evidence (level 5) regarding the effectiveness of robot-assisted UE training using the HandCare system on UE function compared to other interventions during the chronic phase of stroke recovery. However, results from one case study show that UE training using HandCare system is not effective for improving UE function in patients with chronic stroke.
Chronic phase - HapticKnob
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on dexterity among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was no significant improvement in patients’ dexterity (Nine Hole Peg Test) at post-treatment (6 weeks) or follow-up (12 weeks).
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using the HapticKnob system is not effective for improving dexterity in patients with chronic stroke.
Grip Strength
Not Effective
2B
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on grip strength among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was no significant improvement in patients’ grip strength (measured by dynamometry) at post-treatment (6 weeks) or follow-up (12 weeks).
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using the HapticKnob system is not effective for improving grip strength in patients with chronic stroke.
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on hand kinematics among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was a significant improvement in patients’ hand kinematics (hand motor control, motion smoothness and time) at post-treatment (6 weeks).
Note: Kinematic measures were not taken at follow-up (12 weeks).
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using the HapticKnob system is effective for improving hand kinematics in patients with chronic stroke.
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on UE pain among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was no significant change in patients’ UE pain (measured by Visual Analogue Scale) at post-treatment (6 weeks) or follow-up (12 weeks).
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using the HapticKnob system is not effective in reducing UE pain in patients with chronic stroke.
Satisfaction
Not Effective
2B
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on satisfaction among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was no significant improvement in patients’ satisfaction (measured using a 4-point Likert scale) at post-treatment (6 weeks) or follow-up (12 weeks).
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using HapticKnob system is not effective for improving patient satisfaction in the chronic stage of stroke recovery.
Spasticity
Not Effective
2B
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on UE spasticity among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was no significant reduction in patients’ UE spasticity (Modified Ashworth Scale) at post-treatment (6 weeks), but a significant reduction in spasticity was reported at follow-up (12 weeks).
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using the HapticKnob system is not effective in reducing UE spasticity in patients with chronic stroke in the short term.
Note:However, reduced spasticity was noted at follow-up (6 weeks post-treatment).
One pre-post study (Lambercy et al., 2011) investigated the effects of UE robot-assisted training using the HapticKnob system on UE function among patients with chronic stroke. This pre-post study provided patients with chronic stroke with UE robot-assisted training using the HapticKnob device. Robot-assisted training consisted of goal-directed hand opening/closing and forearm pronation/supination exercises. There was a significant improvement in most measures of UE function (Fugl-Meyer Assessment of Upper Extremity total and wrist/hand scores, Motricity Index total and shoulder/elbow scores, Motor Assessment Scale) at post-treatment (6 weeks) and follow-up (12 weeks).
Note: There was no significant improvement in Fugl-Meyer Assessment of Upper Extremity shoulder/elbow scores, Motricity Index hand/finger scores or Functional Test of the Hemiparetic Upper Extremity scores at either time point.
Conclusion: There is limited evidence (level 2b) from one pre-post study that UE training using the HapticKnob system is effective for improving UE function in patients with chronic stroke.
Chronic phase - L-EXOS
Range of motion
Effective
2B
L-EXOS (Light Exoskeleton)
One quasi-experimental study (Frisoli et al., 2009) investigated the effects of UE robot-assisted training using the L-EXOS system on UE ROM among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the L-EXOS device. Training consisted of goal-directed robot-assisted reaching, path following and free motion tasks involving shoulder and elbow joints with an integrated virtual reality system. There was a significant improvement in patients’ shoulder and elbow active ROM at post-treatment (6 weeks).
Note: there were no significant changes in patients’ shoulder and elbow passive ROM at post-treatment.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the L-EXOS system is effective for improving UE active ROM in patients with chronic stroke.
Spasticity
Not Effective
2B
L-EXOS (Light Exoskeleton)
One quasi-experimental study (Frisoli et al., 2009) investigated the effects of UE robot-assisted training using the L-EXOS system on UE spasticity among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the L-EXOS device. Training consisted of goal-directed robot-assisted reaching, path following and free motion tasks involving shoulder and elbow joints with an integrated virtual reality system. There was no significant change in patients’ UE spasticity (Modified Ashworth Scale) at post-treatment (6 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the L-EXOS system is not effective in reducing UE spasticity in patients with chronic stroke.
L-EXOS (Light Exoskeleton)
One quasi-experimental study (Frisoli et al., 2009) investigated the effects of UE robot-assisted training using the L-EXOS system on UE function among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the L-EXOS device. Training consisted of goal-directed robot-assisted reaching, path following and free motion tasks involving shoulder and elbow joints with an integrated virtual reality system. There was a significant improvement in UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (6 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the L-EXOS system is effective for improving UE function in patients with chronic stroke.
Chronic phase - MEMOS
MEMOS (Elbow-shoulder manipulator mechatronic system for motor recovery after stroke)
One quasi-experimental study (Colombo et al., 2010) investigated the effects of UE robot-assisted training using the MEMOS system on UE kinematics among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the MEMOS system. Training consisted of goal-directed active and active-assistive elbow and shoulder reaching movements in the horizontal plane. There was a significant improvement in patients’ movement dynamics (normalized force control parameter and force directional error) at post-treatment (3 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the MEMOS system is effective for improving movement dynamics in patients with chronic stroke.
MEMOS (Elbow-shoulder manipulator mechatronic system for motor recovery after stroke)
One quasi-experimental study (Colombo et al., 2010) investigated the effects of UE robot-assisted training using the MEMOS system on UE strength among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the MEMOS system. Training consisted of goal-directed active and active-assistive elbow and shoulder reaching movements in the horizontal plane. There was an improvement in patients’ UE strength (measured as co-contraction indices of biceps brachii/triceps brachii, anterior/posterior deltoid, and pectoralis major/teres major muscle groups) at post-treatment (3 weeks).
Note: Although an improvement was reported, statistical data was not provided for this outcome.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the MEMOS system is effective for improving UE strength in patients with chronic stroke.
MEMOS (Elbow-shoulder manipulator mechatronic system for motor recovery after stroke)
One quasi-experimental study (Colombo et al., 2010) investigated the effects of UE robot-assisted training using the MEMOS system on UE function among patients with chronic stroke. This quasi-experimental study provided patients with chronic stroke with UE robot-assisted training using the MEMOS system. Training consisted of goal-directed active and active-assistive elbow and shoulder reaching movements in the horizontal plane. There was a significant improvement in patients’ UE function (Fugl-Meyer Assessment of Upper Extremity Function, Motor Status Score) at post-treatment (3 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the MEMOS system is effective for improving UE function in patients with chronic stroke.
Chronic phase - MIME
Functional Independence
Not Effective
1B
MIME (Mirror Image Movement Enabler)
One high quality RCT (Lum et al., 2002) investigated the effects of UE robot-assisted training using the MIME system on functional independence among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the MIME device or conventional neurodevelopmental therapy. Robot-assisted training consisted of forearm and shoulder goal-directed reaching movements in 4 modes: passive, active-assisted, active-constrained and bimanual. There were no significant between-group differences in functional independence (Functional Independence Measure (FIM), Barthel Index) at mid-treatment (1 month) or post-treatment (2 months). While between-group differences in Barthel Scores remained insignificant at follow-up (6 months), there was a significant between-group difference in FIM scores at follow-up in favour of UE robot-assisted training compared to conventional neurodevelopmental therapy.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIME system is not more effective than a comparison intervention (conventional neurodevelopmental therapy) for improving functional independence in patients with chronic stroke.
Note: However, a significant between-group difference in one measure of functional independence was noted at follow-up (6 months post-treatment) in favour of UE robot-assisted training compared to a comparison intervention.
MIME (Mirror Image Movement Enabler)
One high quality RCT (Lum et al., 2002) investigated the effects of UE robot-assisted training using the MIME system on kinematic outcome (reaching extent) among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the MIME device or conventional neurodevelopmental therapy. Robot-assisted training consisted of forearm and shoulder goal-directed reaching movements in 4 modes: passive, active-assisted, active-constrained and bimanual. There was a significant between-group difference in patients’ reach kinematics (forward-lateral and lateral reach at tabletop and shoulder heights; and forward-medial and forward reach at shoulder height) at post-treatment (2 months), in favour of robot-assisted training compared to conventional neurodevelopmental therapy.
Note: Kinematic measures were not reported at mid-treatment (1 month) or follow-up (6 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIME system is more effective than a comparison intervention (conventional neurodevelopmental therapy) for improving reach kinematics in patients with chronic stroke.
MIME (Mirror Image Movement Enabler)
One high quality RCT (Lum et al., 2002) investigated the effects of UE robot-assisted training using the MIME system on UE strength among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the MIME device or conventional neurodevelopmental therapy. Robot-assisted training consisted of forearm ad shoulder goal-directed reaching movements in 4 modes: passive, active-assisted, active-constrained and bimanual. There was a significant between-group difference in UE strength (shoulder flexion, elbow flexion, extension, abduction and adduction) at post-treatment (2 months), in favour of robot-assisted training compared to conventional neurodevelopmental therapy.
Note: Strength measures were not reported at mid-treatment (1 month) or follow-up (6 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIME system is more effective than a comparison intervention (conventional neurodevelopmental therapy) for improving UE strength in patients with chronic stroke.
MIME (Mirror Image Movement Enabler)
One high quality RCT (Lum et al., 2002) investigated the effects of UE robot-assisted training using the MIME system on UE function among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the MIME device or conventional neurodevelopmental therapy. Robot-assisted training consisted of forearm and shoulder goal-directed reaching movements in 4 modes: passive, active-assisted, active-constrained and bimanual. There was a significant between-group difference in UE function (Fugl-Meyer Assessment of Upper Extremity Function shoulder/elbow score) at mid-treatment (1 month) and post-treatment (2 months), in favour of robot-assisted training compared to conventional neurodevelopmental therapy. Results did not remain significant at follow-up (6 months).
Note: There were no significant between-group differences in Fugl-Meyer Assessment of Upper Extremity Function wrist/hand scores at any time point.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIME system is more effective than a comparison intervention (conventional neurodevelopmental therapy) for improving UE function in patients with chronic stroke.
Chronic phase - MIT-Manus
Emotional Wellbeing
Not Effective
1B
One high quality RCT (Volpe et al., 2008) investigated the effects of UE robot-assisted training using the MIT-Manus system on emotional wellbeing among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive intensive UE robot-assisted training or intensive sensorimotor arm training mediated by a therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus InMotion2 device. There was no significant between-group difference in patients’ emotional wellbeing (Beck Depression Scale) at post-treatment (6 weeks) or follow-up (3 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIT-Manus system is not more effective than a comparison intervention (sensorimotor arm training) for improving emotional wellbeing in patients with chronic stroke.
Kinematics
Not Effective
1B
One high quality RCT (Conroy et al., 2011) and two quasi-experimental studies (Zollo et al., 2011; Dipietro et al., 2012) investigated the effects of UE robot-assisted training using the MIT-Manus system on UE kinematics among patients with chronic stroke.
The high quality RCT (Conroy et al., 2011) randomized patients with chronic stroke to receive robot-assisted planar reaching exercises using the MIT-Manus device, robot-assisted planar and vertical reaching exercises using the MIT-Manus device, or intensive conventional arm exercises. There were no significant between-group differences in most reach kinematic measures (Z force, deviation, mean speed, peak speed, smoothness, duration, ellipse ratio) at post-treatment (6 weeks) or follow-up (12 weeks).
Note: There was a significant between-group difference in aim at both time points, in favour of both robot-assisted training groups compared to conventional arm exercises.
The first quasi-experimental study (Zollo et al., 2011) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device (InMotion2 and 3). Training comprised goal-directed planar passive, active-assisted and active tasks that emphasized shoulder, elbow, and wrist movements. There was a significant improvement in UE kinematic and dynamic indices and motion planning indices at post-treatment (12 weeks).
The second quasi-experimental study (Dipietro et al., 2012) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device (InMotion2). Training included point-to-point reaching tasks using elbow and shoulder movements in passive, active-assistive and active modes. There were significant improvements in most kinematic measures (smoothness metrics, movement and submovement metrics) at post-treatment (18 sessions).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIT-Manus system is not more effective than a comparison intervention (conventional arm exercises) for improving UE kinematic outcomes in patients with chronic stroke.
Note: However, two quasi-experimental studies showed significant improvements in kinematic measures after UE training using the MIT-Manus device.
Two high quality RCTs (Volpe et al., 2008; Lo et al., 2010) and one quasi-experimental study (Posteraro et al., 2009) investigated the effects of UE robot-assisted training using the MIT-Manus system on pain among patients with chronic stroke.
The first high quality RCT (Volpe et al., 2008) randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus InMotion2 device. There was no significant between-group difference in UE pain (Fugl-Meyer Assessment of Upper Extremity Function pain score) at post-treatment (6 weeks) or follow-up (3 months).
The second high quality RCT (Lo et al., 2010) randomized patients with chronic stroke to receive intensive robot-assisted therapy using the MIT-Manus device, intensity-matched intensive conventional rehabilitation or usual care. Robot-assisted training consisted of 4 modules: a shoulder-elbow unit for horizontal movements, an antigravity unit for vertical movements, a wrist unit for flexion/extension, abduction/adduction and pronation/supination, and a grasp hand unit for closing and opening movements. There were no significant between-group differences in pain (measured by Visual Analogue Scale) at post-treatment (12 weeks) or follow-up (36 weeks).
The quasi-experimental study (Posteraro et al., 2009) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device. Training comprised goal-directed planar passive and active-assisted reaching tasks that emphasized shoulder and elbow movements. There was no significant change in patients’ UE pain (measured using a 4-point verbal rating scale) at post-treatment (6 weeks) or 3 months (follow-up).
Conclusion: There is moderate evidence (level 1b) from two high quality RCTs and one quasi-experimental study that UE training using the MIT-Manus system is not more effective than comparison interventions (sensorimotor training, conventional rehabilitation, usual care) for reducing UE pain in patients with chronic stroke. Results also imply that UE robot-assisted training using the MIT-Manus device does not cause more pain than comparison interventions.
Range of motion
Not Effective
1B
One high quality RCT (Volpe et al., 2008) and one quasi-experimental study (Posteraro et al., 2009) investigated the effects of UE robot-assisted training using the MIT-Manus system on range of motion (ROM) among patients with chronic stroke.
The high quality RCT (Volpe et al., 2008) randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus In-Motion 2 device. There were no significant between-group differences in UE passive ROM (measured using a 5-point scale) at post-treatment (6 weeks) or follow-up (3 months).
The quasi-experimental study (Posteraro et al., 2009) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device. Training comprised goal-directed planar passive and active-assisted reaching tasks that emphasized shoulder and elbow movements. There were significant improvements in patients’ shoulder and elbow passive ROM at post-treatment (6 weeks), and results for shoulder passive ROM remained significant at follow-up (3 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIT-Manus device is not more effective than a comparison intervention (sensorimotor arm training) for improving passive UE ROM in patients with chronic stroke.
Note: However, a quasi-experimental study reported improved shoulder and elbow passive range of motion following robot-assisted training with the MIT-Manus device.
Shoulder dislocation
Not Effective
1B
One high quality RCT (Volpe et al., 2008) investigated the effects of UE robot-assisted training using the MIT-Manus system on incidence of shoulder dislocation among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus In-Motion 2 device. There was no significant between-group difference in patients’ incidence of shoulder dislocation at post-treatment (6 weeks) or follow-up (3 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the MIT-Manus system is not more effective than a comparison intervention (sensorimotor arm training) for improving the incidence of shoulder dislocation in patients with chronic stroke. Results also imply that UE robot-assisted training using the MIT-Manus device does not cause a greater incidence of shoulder dislocation than comparison interventions.
Spasticity
Not Effective
1A
Two high quality RCTs (Volpe et al., 2008; Lo et al., 2010) and one quasi-experimental study (Posteraro et al., 2009) investigated the effects of UE robot-assisted training using the MIT-Manus device on UE spasticity among patients with chronic stroke.
The first high quality RCT (Volpe et al., 2008) randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus In-Motion 2 device. There were no significant between-group differences in UE spasticity (Modified Ashworth Scale) at post-treatment (6 weeks) or follow-up (3 months).
The second high quality RCT (Lo et al., 2010) randomized patients with chronic stroke to receive intensive robot-assisted therapy using the MIT-Manus device, intensity-matched intensive conventional rehabilitation or usual care. Robot-assisted training consisted of 4 modules: a shoulder-elbow unit for horizontal movements, an antigravity unit for vertical movements, a wrist unit for flexion/extension, abduction/adduction and pronation/supination, and a grasp hand unit for closing and opening movements. There were no significant between-group differences in UE spasticity (Modified Ashworth Scale) at post-treatment (12 weeks) or follow-up (36 weeks).
The quasi-experimental study (Posteraro et al., 2009) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device. Training comprised goal-directed planar passive and active-assisted reaching tasks that emphasized shoulder and elbow movements. There were significant reductions in shoulder spasticity (Modified Ashworth Scale) at post-treatment (6 weeks), but results did not remain significant at follow-up (3 months). There were no significant changes in elbow spasticity (Modified Ashworth Scale) at either time point.
Conclusion: There is strong evidence (level 1a) from two high quality RCTs that UE robot-assisted training using the MIT-Manus system is not more effective than comparison interventions (sensorimotor arm training, conventional rehabilitation, usual care) for reducing UE spasticity in patients with chronic stroke.
Note: However, one quasi-experimental study reported reduced shoulder spasticity following robot-assisted training using the MIT-Manus device, in the short-term only.
One high quality RCT (Volpe et al., 2008) and two quasi-experimental study (MacClellan et al., 2005; Zollo et al., 2011) investigated the effects of UE robot-assisted training using the MIT-Manus system on UE strength among patients with chronic stroke.
The high quality RCT (Volpe et al., 2008) randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus In-Motion 2 device. There were no significant between-group differences in patients’ shoulder or elbow strength (Medical Research Council – MRC, scale of motor power) at midpoint (3 weeks), post-treatment (6 weeks) or follow-up (3 months).
The first quasi-experimental study (MacClellan et al., 2005) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device (InMotion 2). Training comprised goal-directed planar passive, active-assisted and active reaching tasks that emphasized shoulder and elbow movements. There was a significant improvement in UE strength (Motor Power Assessment) among patients with severe stroke impairment (Fugl-Meyer Assessment of Upper Extremity Function score ≤ 15) at post-treatment (4 weeks), but results did not remain significant at follow-up (3 months). There was no significant change in UE strength among patients with moderate stroke impairment (FMA score > 15) at post-treatment or follow-up.
The second quasi-experimental study (Zollo et al., 2011) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device (InMotion 2 and 3). Training comprised goal-directed planar passive, active-assisted and active tasks that emphasized shoulder, elbow, and wrist movements. There was a significant improvement in UE strength (Motor Power Scale) at post-treatment (12 weeks).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE robot-assisted training using the MIT-Manus system is not more effective than a comparison intervention (sensorimotor arm training) for improving UE strength in patients with chronic stroke.
Note: However, two quasi-experimental studies reported improved UE strength following robot-assisted training with the MIT-Manus device.
Stroke severity
Conflicting
4
Three high quality RCTs (Volpe et al., 2008; Lo et al., 2010; Conroy et al., 2011) investigated the effects of UE robot-assisted training using the MIT-Manus system on stroke severity outcomes among patients with chronic stroke.
The first high quality RCT (Volpe et al., 2008) randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by a therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus In-Motion 2 device. There were no significant between-group differences in stroke severity (Stroke Impact Scale, National Institute of Health Stroke Scale) at post-treatment (6 weeks) or follow-up (3 months).
The second high quality RCT (Lo et al., 2010) randomized patients with chronic stroke to receive intensive robot-assisted therapy using the MIT-Manus device, intensity-matched conventional rehabilitation or usual care. Robot-assisted therapy consisted of 4 modules: a shoulder-elbow unit for horizontal movements, an antigravity unit for vertical movements, a wrist unit for flexion/extension, abduction/adduction and pronation/supination; and a grasp hand unit for closing and opening movements. There were significant between-group differences in stroke severity (Stroke Impact Scale) at post-treatment (12 weeks) and follow-up (36 weeks), in favour of robot-assisted therapy compared to usual care. There were no significant differences between robot-assisted therapy and intensity-matched conventional rehabilitation.
The third high quality RCT (Conroy et al., 2011) randomized patients with chronic stroke to receive robot-assisted planar reaching exercises using the MIT-Manus device, robot-assisted planar + vertical reaching exercises using the MIT-Manus device, or intensive conventional arm exercises. At post-treatment (6 weeks) there was a significant between-group difference in one measure of stroke severity (Stroke Impact Scale Activities of Daily Living score), in favour of robot-assisted planar + vertical reach training compared to intensive conventional rehabilitation. There were no significant between-group differences in other measures of stroke severity (Stroke Impact Scale hand and mobility scores) at post-treatment. There were no significant between-group differences in any measure of stroke severity at follow-up (12 weeks).
Note: At post-treatment (6 weeks), a significant between-group difference was also reported in a subgroup of patients with severe impairment (baseline FMA score ≤ 25), in favour of robot-assisted planar + vertical reach training compared with intensive conventional rehabilitation. Results did not remain significant at follow-up.
Conclusion: There is conflicting evidence (level 4) regarding the effect of UE robot-assisted training using the MIT-Manus system compared to other interventions on stroke severity in the chronic phase of stroke recovery. One high quality study found no difference in strokeseverity between robot-assisted training using the MIT-Manus device and sensorimotor training. Another high quality study found that robot-assisted training using the MIT-Manus device was more effective than usual care. A third high quality RCT found robot-assisted training using the MIT-Manus device was more effective than intensive conventional arm exercises for improving strokesymptoms relating to ADLs but not hand function or mobility.
UE function
Not Effective
1A
Three high quality RCTs (Volpe et al., 2008; Lo et al., 2010; Conroy et al., 2011) and three quasi-experimental studies (MacClellan et al., 2005; Posteraro et al., 2009; Zollo et al., 2011) investigated the effects of UE robot-assisted training using the MIT-Manus system on UE function outcomes among patients with chronic stroke.
The first high quality RCT (Volpe et al., 2008) randomized patients with chronic stroke to receive intensive UE robot-assisted training using the MIT-Manus device or intensive sensorimotor arm training mediated by a therapist. Robot-assisted training consisted of planar active and active-assisted goal-directed exercises using the MIT-Manus In-Motion 2 device. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity Function shoulder/elbow or wrist/hand scores) at mid-treatment (3 weeks), post-treatment (6 weeks) or follow-up (3 months).
The second high quality RCT (Lo et al., 2010) randomized patients with chronic stroke to receive intensive robot-assisted therapy using the MIT-Manus device, intensity-matched conventional rehabilitation or usual care. Robot-assisted therapy consisted of 4 modules: a shoulder-elbow unit for horizontal movements, an antigravity unit for vertical movements, a wrist unit for flexion/extension, abduction/adduction and pronation/supination; and a grasp hand unit for closing and opening movements. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity Function, Wolf Motor Function Test) at post-treatment (12 weeks). However, there was a significant between-group difference in both measures of UE function at follow-up (36 weeks) in favour of robot-assisted therapy compared to usual care.
The third high quality RCT (Conroy et al., 2011)randomized patients with chronic stroke to receive robot-assisted planar reaching exercises using the MIT-Manus device, robot-assisted planar + vertical reaching exercises using the MIT-Manus device, or intensive conventional arm exercises. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity Function, Wolf-Motor Function Test) at post-treatment (6 weeks) or follow-up (12 weeks).
The first quasi-experimental study (MacClellan et al., 2005) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device (InMotion 2). Training comprised goal-directed planar passive, active-assisted and active reaching tasks that emphasized shoulder and elbow movements. Analysis of patients with moderate stroke impairment (FMA score > 15) showed no significant improvements in most measures of UE function (Fugl-Meyer Assessment of Upper Extremity Function total, shoulder/elbow and wrist/hand scores, Motor Status Scale shoulder/elbow and wrist/hand scores, Wolf Motor Function Test – performance time scores) at post-treatment (4 weeks) or follow-up (3 months). However, this subgroup did demonstrate a significant improvement in Wolf Motor Function Test – functional ability scores (post-treatment only), and a significant improvement in Fugl-Meyer Assessment of Upper Extremity Function shoulder/elbow scores (follow-up only). Patients with severe stroke impairment (FMA score ≤ 15) showed a significant improvement in Fugl-Meyer Assessment of Upper Extremity Function total and shoulder/elbow scores only at post-treatment (4 weeks). They did not demonstrate significant improvements on any measure of UE function at follow-up (3 months).
The second quasi-experimental study (Posteraro et al., 2009) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device. Training comprised goal-directed planar passive and active-assisted reaching tasks that emphasized shoulder and elbow movements. There were significant improvements in UE function (Motor Status Scale shoulder/elbow scores) at post-treatment (6 weeks), but results did not remain significant at follow-up (3 months).
The third quasi-experimental study (Zollo et al., 2011) provided patients with chronic stroke with UE robot-assisted training using the MIT-Manus device (InMotion 2 and 3). Training comprised goal-directed planar passive, active-assisted and active tasks that emphasized shoulder, elbow, and wrist movements. There was a significant improvement in UE function (Fugl-Meyer Assessment of Upper Extremity Function) at post-treatment (12 weeks).
Conclusion: There is strong evidence (level 1a) from three high quality RCTs that UE robot-assisted training using the MIT-Manus system is not more effective than comparison interventions (sensorimotor arm training, intensity-matched conventional rehabilitation, intensive conventional arm exercises) for improving UE function in patients with chronic stroke.
Note: However, one high quality RCT found that UE robot-assisted training using the MIT-Manus device was more effective than usual care (at follow-up – 36 weeks) for improving UE function in the chronic stage of stroke recovery. Furthermore, three quasi-experimental studies reported improved UE function following robot-assisted training using the MIT-Manus device.
Chronic phase - Pneumatic Glove
One high quality RCT (Connelly et al., 2010) and one fair quality RCT (Fischer et al., 2007) investigated the effects of UE robot-assisted training using a pneumatic glove on dexterity among patients with chronic stroke.
The high quality RCT (Connelly et al., 2010) randomized patients with chronic stroke to receive UE robot-assisted training using the PneuGlove system or UE training without robot assistance. Training consisted of functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in dexterity (Box and Block Test) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
The fair quality RCT (Fischer et al., 2007) randomized patients with chronic stroke to receive UE robot-assisted training using a pneumatic orthosis for automated-assisted digit extension, a cable orthosis for self-assisted digit extension, or no orthosis. Training comprised functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in dexterity (Box and Blocks Test) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCTthat UE training using a pneumatic glove is not more effective than comparison interventions (UE training without robot assistance, UE training using a cable orthosis,or no orthosis) for improving dexterity in patients with chronic stroke.
Grip and pinch strength
Not Effective
1B
One high quality RCT (Connelly et al., 2010) and one fair quality RCT (Fischer et al., 2007) investigated the effects of UE robot-assisted training using a pneumatic glove on grip and pinch strength among patients with chronic stroke.
The high quality RCT (Connelly et al., 2010) randomized patients with chronic stroke to receive UE robot-assisted training using the PneuGlove system or UE training without robot assistance. Robot-assisted training consisted of functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in lateral or palmar pinch strength or grip strength at post-treatment (6 weeks) or follow-up (1 month post-treatment).
The fair quality RCT (Fischer et al., 2007) randomized patients with chronic stroke to receive UE robot-assisted training using a pneumatic orthosis for automated-assisted digit extension, a cable orthosis for self-assisted digit extension, or no orthosis. Training comprised functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in grip strength (measured by dynamometer) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCTthat UE training using a pneumatic glove is not more effective than comparison interventions (UE training without robot assistance, UE training using a cable orthosis, or no orthosis) for improving grip or pinch strength in patients with chronic stroke.
Kinematics
Not Effective
2a
One fair quality RCT (Fischer et al., 2007) investigated the effects of UE robot-assisted training using a pneumatic glove on UE kinematics among patients with chronic stroke. This fair quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using a pneumatic orthosis for automated-assisted digit extension, a cable orthosis for self-assisted digit extension, or no orthosis. Training comprised functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in hand kinematics (peak velocity and flexion/extension isometric strength of the metacarpophalangeal joints) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using a pneumatic glove is not more effective than comparison interventions (UE training using a cable orthosis or no orthosis) for improving hand kinematic outcomes in patients with chronic stroke.
Range of Motion
Not Effective
2A
One fair quality RCT (Fischer et al., 2007) investigated the effects of UE robot-assisted training using a pneumatic glove on UE range of motion (ROM) among patients with chronic stroke. This fair quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using a pneumatic orthosis for automated-assisted digit extension, a cable orthosis for self-assisted digit extension, or no orthosis. Training comprised functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in hand ROM (active extension of metacarpophalangeal joints) at post-treatment (6 weeks) or follow-up (1 month post-treatment).a/p>
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using a pneumatic glove is not more effective than comparison interventions (UE training using a cable orthosis or no orthosis) for improving hand ROM in patients with chronic stroke.
Spasticity
Not Effective
2A
One fair quality RCT (Fischer et al., 2007) investigated the effects of UE robot-assisted training using a pneumatic glove on UE spasticity among patients with chronic stroke. This fair quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using a pneumatic orthosis for automated-assisted digit extension, a cable orthosis for self-assisted digit extension, or no orthosis. Training comprised functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in hand spasticity (metacarpophalangeal joints) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using a pneumatic glove is not more effective than comparison interventions (UE training using a cable orthosis or no orthosis) for managing hand spasticity in patients with chronic stroke.
UE Function
Not Effective
1B
One high quality RCT (Connelly et al., 2010) and one fair quality RCT (Fischer et al., 2007) investigated the effects of UE robot-assisted training using a pneumatic glove on UE function among patients with chronic stroke.
The high quality RCT (Connelly et al., 2010) randomized patients with chronic stroke to receive UE robot-assisted training using the PneuGlove system or UE training without robot assistance. Training consisted of functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity Function total and hand/wrist scores) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
The fair quality RCT (Fischer et al., 2007) randomized patients with chronic stroke to receive UE robot-assisted training using a pneumatic orthosis for automated-assisted digit extension, a cable orthosis for self-assisted digit extension, or no orthosis. Training comprised functional grasp-and-release tasks involving a mixture of virtual objects and actual objects. There were no significant between-group differences in UE function (Wolf Motor Function Test time score, Fugl-Meyer Assessment of the Upper Extremity, Rancho Los Amigos Functional Test of the Hemiparetic Upper Extremity) at post-treatment (6 weeks) or follow-up (1 month post-treatment).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCT that UE training using a pneumatic glove is not more effective than comparison interventions (UE training without robot assistance, UE training using a cable orthosis, or no orthosis) for improving UE function in patients with chronic stroke.
Chronic phase - ReoGo
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on dexterity among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was a significant improvement in dexterity (Box and Block Test) at post-treatment (4 weeks) and follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving dexterity in patients with chronic stroke.
Functional independence
Effective
2B
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on functional independence among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was a significant improvement in patients’ functional independence (Functional Independence Measure motor subscale) at post-treatment (4 weeks) and follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving functional independence in patients with chronic stroke.
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on mobility among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was a significant improvement in patients’ mobility (Time Up and Go Test) at post-treatment (4 weeks) and follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving mobility in patients with chronic stroke.
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on UE pain among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was no significant change in patients’ reported UE pain (measured by visual analogue scale) at post-treatment (4 weeks), but there was a significant improvement in UE pain at follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is not effective for improving UE pain in patients with chronic stroke in the short term.
Note: Changes in UE pain were significant at follow-up.
Quality of life
Not Effective
2B
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on quality of life of patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There were no significant changes in patients’ quality of life (Euro-QoL) at 1 month post-treatment.
Note: Quality of life was not measured at post-treatment (4 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is not effective for improving patients’ quality of life in chronic stroke period.
Satisfaction
Not Effective
2B
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on satisfaction among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There were no significant changes in patients’ satisfaction (measured by Visual Analogue Scale) at post-treatment (4 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using ReoGo device is not effective for improving patient satisfaction in the chronic stroke period.
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on UE spasticity of patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was no significant change in spasticity at the shoulder or wrist (Ashworth Scale) at post-treatment (4 weeks) or follow-up (1 month post-treatment). However, there was a significant improvement in spasticity at the elbow at both time points.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for managing spasticityat the elbow (but not the shoulder or wrist) among patients with chronic stroke.
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on UE muscle strength among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was a significant improvement in muscle strength of the trapezius, deltoid, pectoralis major, biceps, internal rotator and latissimus dorsi muscles (Medical Research Council – MRC, scale of motor power) at post-treatment (4 weeks). At follow-up (1 month post-treatment) results remained significant for these muscles and a significant improvement was also reported for triceps and wrist flexors/extensor muscles.
Note: At post-treatment there were no significant improvements in strength of the triceps, external rotator or wrist flexors/extensor muscles. At follow-up there remained no significant improvement in strength of the external rotator muscles.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving UE muscle strength in patients with chronic stroke.
One quasi-experimental study (Bovolenta et al., 2011) investigated the effects of UE robot-assisted training using the ReoGo device on UE function among patients with chronic stroke. This quasi-experimental study assigned patients with chronic stroke to receive UE robot-assisted training using the ReoGo device. Intervention consisted of goal-directed, paretic elbow and shoulder reaching passive and active movements. There was a significant improvement in UE function (Fugl-Meyer Assessment of the Upper Extremity, Frenchay Arm Test) at post-treatment (4 weeks) and follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving UE function in patients with chronic stroke.
Chronic phase - REHAROB
Functional independence
Effective
2B
One poor quality RCT (Fazekas et al., 2007) investigated the effects of UE robot-assisted training using the REHAROB system on UE spasticity among patients with chronic stroke. This poor quality RCT randomized patients with chronic stroke to received UE robot-assisted training using the REHAROB device or UE training without robot assistance. Physiotherapy robot-assisted training consisted of shoulder and elbow exercises executed slowly and with constant velocity in a high repetition number. Patients who received UE robot-assisted training demonstrated a significant reduction in spasticity of the shoulder adductors and elbow flexors (Modified Ashworth Scale) at post-treatment (4 weeks). Significant improvements in UE spasticity were not seen in the control group.
Note: Between-group analyses were not performed.
Conclusion: There is limited evidence (level 2b) from one poor quality RCT that UE training using REHAROB system is effective in managing UE spasticity in patients with chronic stroke.
Range of Motion
Effective
2B
One poor quality RCT (azekas et al., 2007F) investigated the effects of UE robot-assisted training using the REHAROB system on UE ROM of patients with chronic stroke. This poor quality RCT randomized patients with chronic stroke to received UE robot-assisted training using the REHAROB device or UE training without robot assistance. Physiotherapy robot-assisted training consisted of shoulder and elbow exercises executed slowly and with constant velocity in a high repetition number. While neither group demonstrated a significant improvement in shoulder ROM (Fugl-Meyer Assessment of Upper Extremity – shoulder/elbow score), both groups demonstrated a significant improvement in elbow ROM at post-treatment (4 weeks).
Note: Between-group analyses were not performed.
Conclusion: There is limited evidence (level 2b) from one poor quality RCT that UE training using the REHAROB system is effective for improving elbow ROM (but not shoulder ROM) of patients with chronic stroke.
One poor quality RCT (Fazekas et al., 2007) investigated the effects of UE robot-assisted training using the REHAROB system on UE spasticity among patients with chronic stroke. This poor quality RCT randomized patients with chronic stroke to received UE robot-assisted training using the REHAROB device or UE training without robot assistance. Physiotherapy robot-assisted training consisted of shoulder and elbow exercises executed slowly and with constant velocity in a high repetition number. Patients who received UE robot-assisted training demonstrated a significant reduction in spasticity of the shoulder adductors and elbow flexors (Modified Ashworth Scale) at post-treatment (4 weeks). Significant improvements in UE spasticity were not seen in the control group.
Note: Between-group analyses were not performed.
Conclusion: There is limited evidence (level 2b) from one poor quality RCT that UE training using REHAROB system is effective in managing UE spasticity in patients with chronic stroke.
One poor quality RCT (Fazekas et al., 2007) investigated the effects of UE robot-assisted training using the REHAROB system on UE function among patients with chronic stroke. This poor quality RCT randomized patients with chronic stroke to received UE robot-assisted training using the REHAROB device or UE training without robot assistance. Physiotherapy robot-assisted training consisted of shoulder and elbow exercises executed slowly and with constant velocity in a high repetition number. Both groups demonstrated a significant improvement in UE function (Fugl-Meyer Assessment of the Upper Extremity Function shoulder/elbow score, Rivermead Motor Assessment arm score) at post-treatment (4 weeks).
Note: Between-group analyses were not performed.
Conclusion: There is limited evidence (level 2b) from one poor quality RCT that UE training using REHAROB system is effective for improving UE function in patients with chronic stroke.
Chronic phase - T-WREX / Pneu-WREX
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One high quality RCT (Reinkensmeyer et al., 2012) investigated the effects of UE robot-assisted training using the Pneu-WREX system on dexterity among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the Pneu-WREX device or conventional tabletop therapy. All patients crossed over to the other group for 30 minutes weekly; therefore, each group overall experience 84% of their primary therapy and 16% of the other therapy. The Pneu-WREX device provides passive arm support that allows for elbow flexion/extension, shoulder abduction/adduction, shoulder flexion/extension and shoulder forward-backward translation. There were no significant between-group differences in dexterity (Box and Block Test) at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using Pneu-WREX system is not more effective than conventional rehabilitation for improving dexterity in patients with chronic stroke.
Grip strength
Not Effective
1b
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One high quality RCT (Reinkensmeyer et al., 2012) and one fair quality RCT (Housman et al., 2009) investigated the effects of UE robot-assisted training using the T-WREX or Pneu-WREX systems on grip strength among patients with chronic stroke.
The high quality RCT (Reinkensmeyer et al., 2012) randomized patients with chronic stroke to receive robot-assisted upper extremity training using the Pneu-WREX device or conventional tabletop therapy. All patients crossed over to the other group for 30 minutes weekly; therefore, each group overall experience 84% of their primary therapy and 16% of the other therapy. The Pneu-WREX device provides passive arm support that allows for elbow flexion/extension, shoulder abduction/adduction, shoulder flexion/extension and shoulder forward-backward translation. There were no significant between-group differences in grip strength (Jamar Hand Dynamometer) at post-treatment (8-9 weeks) or follow-up (6 months).
The fair quality RCT (Housman et al., 2009) randomized patients with chronic stroke to receive UE robot-assisted training using the T-WREX device or conventional rehabilitation. Robot-assisted training used the passive arm orthosis while playing computer games in a gravity-supported environment. There were no significant between-group differences in grip strength (measured by dynamometry) at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCTthat UE training using T-WREX or Pneu-WREX systems is not more effective than conventional rehabilitation for improving grip strength in patients with chronic stroke.
Kinematics
Not Effective
2A
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One fair quality RCT (Housman et al., 2009) investigated the effect of UE robot-assisted training using the T-WREX system on UE kinematics among patients with chronic stroke. This fair quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the T-WREX device or conventional rehabilitation. Robot-assisted training used the passive arm orthosis while playing computer games in a gravity-supported environment. There were no significant between-group differences in UE kinematics (free reaching) at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using the T-WREX system is not more effective than conventional rehabilitation for improving UE kinematic outcomes in patients with chronic stroke.
Range of Motion
Not Effective
2a
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One fair quality RCT (Housman et al., 2009) investigated the effect of UE robot-assisted training using the T-WREX system on UE ROM among patients with chronic stroke. This fair quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the T-WREX device or conventional rehabilitation. Robot-assisted training used the passive arm orthosis while playing computer games in a gravity-supported environment. There were no significant between-group differences in UE ROM at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using the T-WREX system is not more effective than conventional rehabilitation for improving UE ROM in patients with chronic stroke.
Satisfaction
Not Effective
2A
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One fair quality RCT (Housman et al., 2009) investigated the effect of UE robot-assisted training using the T-WREX system on satisfaction among patients with chronic stroke. This fair quality RCT randomized patients with chronic stroke to receive UE robot-assisted training using the T-WREX device or conventional rehabilitation. Robot-assisted training used the passive arm orthosis while playing computer games in a gravity-supported environment. There were no significant between-group differences in patient satisfaction (non-standardized survey) at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is limited evidence (level 2a) from one fair quality RCT that UE training using T-WREX system is not more effective than conventional rehabilitation for improving patient satisfaction in the chronic stage of stroke recovery.
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One high quality RCT (Reinkensmeyer et al., 2012) investigated the effect of UE robot-assisted training using the Pneu-WREX system on UE sensation among patients with chronic stroke. This high quality RCT randomized patients with chronic stroke to receive robot-assisted upper extremity training using the Pneu-WREX device or conventional tabletop therapy. All patients crossed over to the other group for 30 minutes weekly; therefore, each group overall experience 84% of their primary therapy and 16% of the other therapy. The Pneu-WREX device provides passive arm support that allows for elbow flexion/extension, shoulder abduction/adduction, shoulder flexion/extension and shoulder forward-backward translation. There were no significant between-group differences in UE sensation (Nottingham Sensory Assessment) at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that UE training using the Pneu-WREX system is not more effective than conventional rehabilitation for improving UE sensation in patients with chronic stroke.
UE Function
Not Effective
1B
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One high quality RCT (Reinkensmeyer et al., 2012) and one fair quality RCT (Housman et al., 2009) investigated the effect of UE robot-assisted training using the Pneu-WREX or T-WREX systems on UE function among patients with chronic stroke.
The high quality RCT (Reinkensmeyer et al., 2012) randomized patients with chronic stroke to receive robot-assisted upper extremity training using the Pneu-WREX device or conventional tabletop therapy. All patients crossed over to the other group for 30 minutes weekly; therefore, each group overall experience 84% of their primary therapy and 16% of the other therapy. The Pneu-WREX device provides passive arm support that allows for elbow flexion/extension, shoulder abduction/adduction, shoulder flexion/extension and shoulder forward-backward translation. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of Upper Extremity Function, Rancho Los Amigos Functional Test for the Hemiparetic Upper Extremity) at post-treatment (8-9 weeks) or follow-up (6 months).
The fair quality RCT (Housman et al., 2009) randomized patients with chronic stroke to receive UE robot-assisted training using the T-WREX device or conventional rehabilitation. Robot-assisted training used the passive arm orthosis while playing computer games in a gravity-supported environment. There were no significant between-group differences in UE function (Fugl-Meyer Assessment of the Upper Extremity Function, Rancho Los Amigos Functional Test for the Hemiparetic Upper Extremity) at post-treatment (8-9 weeks). At follow-up (6 months) there was a significant between-group difference in Fugl-Meyer Assessment scores only, in favour of UE robot-assisted training compared to conventional rehabilitation.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCTthat UE training using the T-WREX and Pneu-WREX systems is not more effective than conventional rehabilitation for improving UE function in patients with chronic stroke.
Note: However, the fair quality RCT reported a significant difference in one measure of UE function at 6-month follow-up, in favour of UE robot-assisted training compared to conventional rehabilitation.
UE Motor Activity
Not Effective
1B
T-WREX (Therapy Wilmington Robotic Exoskeleton) / Pneu-WREX
One high quality RCT (Reinkensmeyer et al., 2012) and one fair quality RCT (Housman et al., 2009) investigated the effect of UE robot-assisted training using the Pneu-WREX or T-WREX systems on UE motor activity among patients with chronic stroke.
The high quality RCT (Reinkensmeyer et al., 2012) randomized patients with chronic stroke to receive robot-assisted upper extremity training using the Pneu-WREX device or conventional tabletop therapy. All patients crossed over to the other group for 30 minutes weekly; therefore, each group overall experience 84% of their primary therapy and 16% of the other therapy. The Pneu-WREX device provides passive arm support that allows for elbow flexion/extension, shoulder abduction/adduction, shoulder flexion/extension and shoulder forward-backward translation. There were no significant between-group differences in UE motor activity (Motor Activity Log – Amount of Use and Quality of Movement scores) at post-treatment (8-9 weeks) or follow-up (6 months).
The fair quality RCT (Housman et al., 2009) randomized patients with chronic stroke to receive UE robot-assisted training using the T-WREX device or conventional rehabilitation. Robot-assisted training used the passive arm orthosis while playing computer games in a gravity-supported environment. There were no significant between-group differences in UE motor activity (Motor Activity Log – Amount of Use and Quality of Movement scores) at post-treatment (8-9 weeks) or follow-up (6 months).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT and one fairquality RCTthat UE training using the Pneu-WREX or T-WREX systems is not more effective than conventional rehabilitation for improving UE motor activity in patients with chronic stroke.
Phase of stroke recovery not specific to one period - GENTLE/S
One study of single-case series (Coote et al., 2008) investigated the effect of UE robot-assisted training using the GENTLE/S system on UE pain among patients with subacute and chronic stroke. This study of 20 single-case series adopted a multiple baseline model to randomize patients with subacute and chronic stroke to receive robot-assisted UE training using the GENTLE/S system, sling suspension UE training or no intervention using an ABC/ACB intervention design. Robot-mediated training comprised reaching and withdrawal movements within a virtual environment in passive, active assisted and active modes. There were no significant differences in patients’ UE pain (measured by Visual Analogue Scale) at the end of each 3-week phase.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than comparison interventions (sling suspension UE training, no UE training) for improving UE pain in patients with subacute and chronic stroke.
Range of motion
Not Effective
2B
One study of single-case series (Coote et al., 2008) investigated the effect of UE robot-assisted training using the GENTLE/S system on UE range of motion (ROM) among patients with subacute and chronic stroke. This study of 20 single-case series adopted a multiple baseline model to randomize patients with subacute and chronic stroke to receive robot-assisted UE training using the GENTLE/S system, sling suspension UE training or no intervention using an ABC/ACB intervention design. Robot-mediated training comprised reaching and withdrawal movements within a virtual environment in passive, active assisted and active modes. There were no significant differences in active ROM on shoulder flexion at the end of each 3-week phase.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than comparison interventions (sling suspension UE training, no UE training) for improving UE ROM in patients with subacute and chronic stroke.
One study of single-case series (Coote et al., 2008) investigated the effect of UE robot-assisted training using the GENTLE/S system on UE sensation among patients with subacute and chronic stroke. This study of 20 single-case series adopted a multiple baseline model to randomize patients with subacute and chronic stroke to receive robot-assisted UE training using the GENTLE/S system, sling suspension UE training or no intervention using an ABC/ACB intervention design. Robot-mediated training comprised reaching and withdrawal movements within a virtual environment in passive, active assisted and active modes. There were no significant differences in UE sensation (Nottingham Sensory Assessment) at the end of each 3-week phase.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than comparison interventions (sling suspension UE training, no UE training) for improving UE sensation in patients with subacute and chronic stroke.
Spasticity
Not Effective
2B
One study of single-case series (Coote et al., 2008) investigated the effect of UE robot-assisted training using the GENTLE/S system on UE spasticity among patients with subacute and chronic stroke. This study of 20 single-case series adopted a multiple baseline model to randomize patients with subacute and chronic stroke to receive robot-assisted UE training using the GENTLE/S system, sling suspension UE training or no intervention using an ABC/ACB intervention design. Robot-mediated training comprised reaching and withdrawal movements within a virtual environment in passive, active assisted and active modes. There were no significant differences in UE spasticity (Modified Ashworth Scale) at the end of each 3-week phase.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than comparison interventions (sling suspension UE training, no UE training) for improving UE spasticityin patients with subacute and chronic stroke.
UE function
Not Effective
2B
One study of single-case series (Coote et al., 2008) investigated the effect of UE robot-assisted training using the GENTLE/S system on UE function among patients with subacute and chronic stroke This study of 20 single-case series adopted a multiple baseline model to randomize patients with subacute and chronic stroke to receive robot-assisted UE training using the GENTLE/S system, sling suspension UE training or no intervention using an ABC/ACB intervention design. Robot-mediated training comprised reaching and withdrawal movements within a virtual environment in passive, active assisted and active modes. There were no significant differences in patients’ UE function (Fugl Meyer Assessment of Upper Extremity Function) at the end of each 3-week phase. However, there was a significant between-group difference in another measure of UE function (Motor Assessment Scale), in favour of robot-mediated therapy compared to sling suspension exercises.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than no UE training for improving UE function in patients with subacute and chronic stroke.
Note: However, results from one measure of UE function indicate that UE training using the GENTLE/S system was more effective than a comparison intervention (sling suspension UE training) for improving UE function of patients.
Unilateral spatial neglect
Not Effective
2B
One study of single-case series (Coote et al., 2008) investigated the effect of UE robot-assisted training using the GENTLE/S system on unilateral spatial neglect (USN) among patients with subacute and chronic stroke. This study of 20 single-case series adopted a multiple baseline model to randomize patients with subacute and chronic stroke to receive robot-assisted UE training using the GENTLE/S system, sling suspension UE training or no intervention using an ABC/ACB intervention design. Robot-mediated training comprised reaching and withdrawal movements within a virtual environment in passive, active assisted and active modes. There were no significant differences in unilateral spatial neglect (Star Cancellation Test) at the end of each 3-week phase.
Conclusion: There is limited evidence (level 2b) from one study of single-case series that UE training using the GENTLE/S system is not more effective than comparison interventions (sling suspension UE training or no UE training) for improving unilateral spatial neglect in patients with subacute and chronic stroke.
Phase of stroke recovery not specific to one period - Robot-Assisted Individual Finger Rehabilitation
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on dexterity among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was no significant between-group difference in dexterity (Nine Hole Peg Test) at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) or 1-month follow-up.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is not more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving dexterity in patients with subacute and chronic stroke.
Grasp and Pinch Strength
Effective
1B
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on grasp and pinch strength among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was a significant between-group difference in grasp and pinch strength at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) and at 1-month follow-up, in favour of robot-assisted finger rehabilitation.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving grasp and pinch strength in patients with subacute and chronic stroke.
Hand Function
Not Effective
1B
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on hand function among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was no significant between-group difference in hand function (Jebsen Taylor Hand Function Test) at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) or 1-month follow-up.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is not more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving hand function in patients with subacute and chronic stroke.
Range of motion
Effective
1B
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on UE ROM among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was a significant between-group difference in active ROM of the second metacarpophalangeal joint at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) and 1-month follow-up, in favour of robot-assisted finger rehabilitation.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving active ROM of the hand in patients with subacute and chronic stroke.
Spasticity
Not Effective
1B
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on UE spasticity among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was no significant between-group difference in spasticity at the elbow or wrist (Ashworth Scale) at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) or 1-month follow-up.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is not more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving UE spasticity in patients with subacute and chronic stroke.
Stroke outcomes
Not Effective
1B
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on stroke outcomes among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was no significant between-group difference in stroke outcomes (Stroke Impact Scale) at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) or 1-month follow-up.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is not more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving strokeoutcomes in patients with subacute and chronic stroke.
One high quality RCT (Hwang et al., 2012) investigated the effects of UE robot-assisted training on UE function among patients with subacute and chronic stroke. This high quality RCT randomized patients with subacute and chronic stroke to receive robot-assisted individual finger rehabilitation for 4 weeks, or early passive therapy for 2 weeks followed by robot-assisted individual finger rehabilitation for 2 weeks. Robot-assisted individual finger rehabilitation consisted of goal-directed, passive, active-assisted and active grasp and release training using virtual reality. There was a significant between-group difference in UE distal function (Fugl-Meyer Assessment of Upper Extremity Function wrist/hand score) at 2 weeks (i.e. robot-assisted training vs. passive therapy), 4 weeks (i.e. robot-assisted training vs. passive therapy + robot-assisted training) and 1-month follow-up, in favour of robot-assisted finger rehabilitation. There was no significant between-group difference in UE proximal function (Fugl-Meyer Assessment of Upper Extremity Function shoulder/elbow score) at any time point.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted individual finger rehabilitation training is more effective than comparison interventions (passive therapy, passive therapy + robot-assisted training) for improving UE distal function (but not proximal function) in patients with subacute and chronic stroke.
Phase of stroke recovery not specific to one period - ReoGo
One quasi-experimental study (Bovolenta et al., 2009) investigated the effect of UE robot-assisted training using the ReoGo device on dexterity among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. There was a significant improvement in dexterity (Box and Block Test) at post-treatment (4 weeks) and follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving dexterity in patients with subacute or chronic stroke.
Functional independence
Effective
2B
One quasi-experimental study (Bovolenta et al., 2009) investigated the effect of UE robot-assisted training using the ReoGo device on functional independence among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. There was a significant improvement in functional independence (Functional Independence Measure motor subscale) at post-treatment (4 weeks) and follow-up (1 month post-treatment), and from post-treatment to follow-up.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental studythat UE training using the ReoGo device is effective for improving functional independence in patients with subacute or chronic stroke.
One quasi-experimental study (Bovolenta et al., 2009) investigated the effect of UE robot-assisted training using the ReoGo device on mobility among patients with subacute or chronic stroke. Thisquasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. While there was no significant improvement in mobility (Timed Up and Go test) at post-treatment (4 weeks), there was a significant improvement at follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is not effective for improving mobility in patients with subacute or chronic strokein the short term.
Note: However, significant improvements in mobility were seen at follow-up.
One quasi-experimental study (Bovolenta et al., 2009) investigated the effects of UE robot-assisted training using the ReoGo device on UE pain among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. While there was no significant improvement in patients’ pain (measured by Visual Analogue Scale) at post-treatment (4 weeks), there was a significant improvement in pain at follow-up (1 month post-treatment).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using ReoGo device is not effective for improving UE pain in patients with subacute or chronic strokein the short term.
Note: However, there was a significant improvement in reported pain at follow-up.
Quality of Life
Not Effective
2B
One quasi-experimental study (Bovolenta et al., 2009) investigated the effect of UE robot-assisted training using the ReoGo device on quality of life among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. There was no significant improvement in patients’ quality of life (Euro-QoL) at 1 month post-treatment.
Note: Quality of life was not measured at post-treatment (4 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is not effective for improving patients’ quality of life in the subacute or chronic strokeperiods.
Satisfaction
Not Effective
2B
One quasi-experimental study (Bovolenta et al., 2009) investigated the effects of UE robot-assisted training using the ReoGo device on treatment satisfaction among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. There were no significant changes in patients’ satisfaction (Visual Analogue Scale) at post-treatment (4 weeks).
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is not effective for improving treatment satisfaction among patients with subacute or chronic stroke.
One quasi-experimental study (Bovolenta et al., 2009) investigated the effects of UE robot-assisted training using the ReoGo device on UE spasticity among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. There was a significant improvement in elbow spasticity (Ashworth Scale) at post-treatment (4 weeks) and 1 month follow-up. There were no significant changes in spasticity at the shoulder or wrist (Ashworth Scale) at either time point.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using ReoGo device is effective for improving spasticityat the elbow (but not the shoulder or wrist) in patients with subacute or chronic stroke.
One quasi-experimental study (Bovolenta et al., 2009) investigated the effect of UE robot-assisted training using the ReoGo device on UE muscle strength among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. At post-treatment (4 weeks) there was a significant improvement in muscle strength of the deltoid, pectoral and biceps muscles (Medical Research Council scale of motor power), but not the trapezius, internal/external rotators, triceps, wrist flexors/extensors or latissimus dorsi muscles. At follow-up (1 month post-treatment) changes in strength were significant for the trapezius, deltoid, pectoralis, biceps, triceps, wrist extensors and latissimus dorsi muscles, but not the internal/external rotator or wrist flexor muscles.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using the ReoGo device is effective for improving UE muscle strength in patients with subacute or chronic stroke.
One quasi-experimental study (Bovolenta et al., 2009) investigated the effects of UE robot-assisted training using the ReoGo device on UE function among patients with subacute or chronic stroke. This quasi-experimental study assigned patients with subacute or chronic stroke to receive UE robot-assisted training using the ReoGo device. The intervention consisted of goal-directed, paretic elbow and shoulder passive and active reaching movements. There was a significant improvement in patients’ UE function (modified Fugl-Meyer Assessment of Upper Extremity, Frenchay Arm Test) at post-treatment (4 weeks) and 1-month follow-up.
Note: UE function was also measured using the ABILHAND at 1-month follow-up. There were no significant changes in ABILHAND scores at this time point.
Conclusion: There is limited evidence (level 2b) from one quasi-experimental study that UE training using ReoGo device is effective in managing UE function in patients with subacute or chronic stroke.
Phase of stroke recovery not specific to one period - UE Robot-Assisted Training
One high quality RCT (Abdullah et al., 2011) investigated the effect of UE robot-assisted training on UE pain among patients with acute and subacute stroke. This high quality RCT randomized patients with acute and subacute stroke to receive robot-assisted UE training or conventional rehabilitation. Robot-assisted training used a 5 degree-of-freedom end-effector device during trajectory and object manipulation exercises incorporating vertical and horizontal, passive, active-assisted and active movements. There was no significant between-group difference in UE pain (Chedoke McMaster Stroke Assessment of Arm and Hand pain inventory score) at post-treatment (8-11 weeks).
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted UE training is not more effective than conventional rehabilitation for improving UE pain in patients with acute and subacute stroke.
Satisfaction
Not Effective
1B
One high quality RCT (Abdullah et al., 2011) investigated the effect of UE robot-assisted training on patient satisfaction in the acute and subacute stages of stroke recovery. This high quality RCT randomized patients with acute and subacute stroke to receive robot-assisted UE training or conventional rehabilitation. Robot-assisted training used a 5 degree-of-freedom end-effector device during trajectory and object manipulation exercises incorporating vertical and horizontal, passive, active-assisted and active movements. There was no significant between-group difference in patient satisfaction (measured according to enjoyment and improvement using 10-point Likert scales) at post-treatment (8-11 weeks).
Conclusion: There is moderate evidence (level 1b) from one high quality RCTthat robot-assisted UE training is not more effective than conventional rehabilitation for improving patient satisfaction in the acute and subacute stages of strokerecovery.
One high quality RCT (Abdullah et al., 2011) investigated the effect of UE robot-assisted training on UE function among patients with acute and subacute stroke. This high quality RCT randomized patients with acute and subacute stroke to receive robot-assisted UE training or conventional rehabilitation. Robot-assisted training used a 5 degree-of-freedom end-effector device during trajectory and object manipulation exercises incorporating vertical and horizontal, passive, active-assisted and active movements. There was a significant between-group difference in UE function (Chedoke McMaster Stroke Assessment of Arm and Hand arm score and hand score) at post-treatment (8-11 weeks), in favour of robot-assisted UE training compared to conventional rehabilitation.
Note: UE function was also measured using the Chedoke Arm and Hand Activity Inventory; no significant between-group differences were seen using this measure at post-treatment.
Conclusion: There is moderate evidence (level 1b) from one high quality RCT that robot-assisted UE training is more effective than conventional rehabilitation for improving UE function in patients with acute and subacute stroke.
References
Abdullah, H.A., Tarry, C., Lambert, C., Barreca, S., & O Allen, B. (2011). Results of clinicians using a therapeutic robotic system in an inpatient strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. rehabilitation unit. Journal of NeuroEngineering and Rehabilitation, 8(50), 1-12.
Aisen, M.L., Krebs, H.I., Hogan, N., McDowell, F., & Volpe, B.T. (1997). The effect of robot-assisted therapy and rehabilitative training on motor recovery following strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Archives of Neurology, 54, 443-6.
Amirabdollahian, F., Loureiro, R., Gradwell, E., Collin, C., Harwin, W., & Johnson, G. (2007). Multivariate analysis of the Fugl-Meyer outcome measures assessment the effectiveness of GENTLE/S robot-mediated strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. therapy. Journal of NeuroEngineering and Rehabilitation, 4, 1-16.
Bovolenta, F., Goldoni, M., Clerici, P., Agosti, M., & Franceschini, M. (2009). Robot therapy for functional recovery of the upper limbs: a pilot study on patients after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Journal of Rehabilitation Medicine, 41, 971-5.
Bovolenta, F., Sale, P., Dall’Armi, V., Clerici, P., & Franceschini, M. (2011). Robot-aided therapy for upper limbs in patients with stroke-related lesions. Brief report of a clinical experience. Journal of NeuroEngineering and Rehabilitation, 8(18), 1-6.
Casadio, C., Giannoni, P., Morasso, P., & Sanguineti, V. (2008). A proof of concept study for the integration of robot therapy with physiotherapy in the treatment of strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients. Clinical Rehabilitation, 23, 217-28.
Chang, J-J., Tung, W-L., Wu, W-L., Huang, M-H., & Su, F-C. (2007). Effects of robot-aided bilateral force-induced isokinetic arm training combined with conventional rehabilitation on arm motor function in patients with chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Archives of Physical Medicine and Rehabilitation, 88, 1332-8.
Colombo, R., Sterpi, I., Mazzone, A., Delconte, C., Minuco, G., & Pisano, F. (2010). Measuring changes of movement dynamics during robot-aided neurorehabilitation of strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients. IEEE Transaction on Neural Systems and Rehabilitation Engineering, 18(1), 75-85.
Coote, S., Murphy, B., Harwin, W., & Stokes, E. (2008). The effect of the GENTLE/s robot-mediated therapy system on arm function after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Clinical Rehabilitation, 22, 395-405.
Connelly, L., Jia, Y., Toro, M.L., Stoykov, M.E., Kenyon, R.V., & Kamper, D.G. (2010). A pneumatic glove and immersive virtual reality environment for hand rehabilitative training after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 18(5), 551-9.
Conroy, S.S., Whitall, J., Sipietro, L., Jones-Lush, L.M., Zhan, M., Finley, M.A., Wittenberg, G.F., Krebs, H.I., & Bever, C.T. (2011). Effects of gravity on robot-assisted motor training after chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a randomized trial. Archives of Physical Medicine and Rehabilitation, 92, 1754-61.
Dipietro, L., Krebs, H.I., Volpe, B.T., Stein, J., Bever, C., Mernoff, S.T., Fasoli, S.E., & Hogan, N. (2012). Learning, not adaptation, characterizes strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. motor recovery: evidence from kinematic changes induced by robot-assisted therapy in rained and untrained task in the same work space. IEEE Transaction on Neural Systems and Rehabilitation Engineering, 20(1), 48-57.
Dovat, L., Lambercy, O., Salman, B., Johnson, V., Milner, T., Gassert, R., Burdet, E., & Leong, T.C. (2010). A technique to train finger coordination and independence after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Disability and Rehabilitation: Assistive Technology, 5(4), 279-87.
Fasoli, S.E., Krebs, H.I., Ferraro, M., Hogan, N., & Volpe, B.T. (2004). Does shorter rehabilitation limit potential recovery poststroke? Neurorehabiltation and Neural Repair, 18, 88-94.
Fazekas, G., Horvath, M., Troznai, T., & Troth, A. (2007). Robot-mediated upper limb physiotherapy for patients with spastic hemiparesis: a preliminary study. Journal of Rehabilitation Medicine, 39, 580-2.
Fischer, H.C., Stubblefield, K., Kline, T., Luo, X., Kenyon, R.V., & Kamper, D.G. (2007). Hand rehabilitation following strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a pilot study of assisted finger extension training in a virtual environment. Topics in StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. Rehabilitation, 14(1), 1-12.
Frisoli, A., Bergamasco, M, Borelli, L., Montagner, A., Greco, G., Procopio, C., Carboncini, M.C., & Rossi, B. (2009). Robotic assisted rehabilitation in virtual reality with the L-EXOS. Study Health Technology Information Journal, 145, 40-54.
Hesse, S., Shulte-Tigges, G., Konrad, M., Bardeleben, A., & Werner, C. (2003). Robot-assisted arm trainer for the passive and active practice of bilateral forearm and wrist movements in hemiparetic subjects. Archives of Physical Medicine and Rehabilitation, 84, 15-20.
Housman, S.J., Scott, K.M., & Reinkensmeyer, D.J. (2009). A randomized controlled trial of gravity-supported, computer-enhanced arm exercise for individual with severe hemiparesis. Neurorehabilitation and Neural Repair, 23, 505-14.
Hu, X.L., Tong, K.Y., Song, R., Tsang, V.S., Leung, P.O. & Le Li, B. (2007). Variation of muscle coactivation patterns in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. during robot-assisted elbow training. Archives of Physical Medicine and Rehabilitation, 88, 1022-9.
Hu, X.L., Tong, K.Y., Song, R., Zheng, X.J., Lui, K.H., Leung, W.W.F., Ng, S., & Au-Yeung, S.S.Y. (2009). Quantitative evaluation of motor functional recovery process in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients during robot-assisted writ training. Journal of Electromyography and Kinesiology, 19, 639-50.
Hwang, C.H., Seong, J.W., & Son, D-S. (2012). Individual finger synchronized robot-assisted hand rehabilitation in subacute to chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a prospective randomized clinical trial of efficacy. Clinical Rehabilitation, 26(8), 696-704.
Kahn, L.E., Zygman, M.L., Rymer, W.Z., Reinkensmeyer, D.J. (2006). Robot-assisted reaching exercise promotes arm movement recovery in chronic hemiparetic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a randomized controlled pilot study. Journal of NeuroEngineering and Rehabilitation, 3, 1-13.
Kahn, L.E., Averbuch, M., Rymer, W.Z., & Reinkensmeyer, J. (2001). Comparison of robot-assisted reaching to free reaching in promoting recovery from chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. In: Mokhtari M, ed. Integration of Assistive Technology in the Information Age. Amsterdam, The Netherlands: IOS Press: 39-44.
Krebs, H.I., Ferraro, M., Buerger, S.P., Newbery, M.J., Makiyama, A., Sandmann, M., Lynch, D., Volpe, B.T., & Hogan, N. (2004). Rehabilitation robotics: pilot trial of a spatial extension for MIT-Manus. Journal of NeuroEngineering and Rehabilitation, 1, 5.
Lambercy, O., Dovat, L., Yun, H., Wee, S.K., Kuah, C.WK., Chua, K. SG., Gassert, R., Milner, T.E., Teo, C.L., & Burdet, E. (2011). Effects of a robot-assisted training of grasp and pronation/supination in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a pilot study. Journal of NeuroEngineering and Rehabilitation, 8, 63.
Liao, W., WU, C., Hsieh, Y., Lin, K., & Chang, W. (2011). Effects of robot-assisted upper limb rehabilitation on daily function and real-world arm activity in patients with chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a randomized controlled trial. Clinical Rehabilitation, 26(2), 111-20.
Lo, A.C., Guarino, P.D., Richards, L.G., Haselkorn, J.K., Wittenberg, G.F., Federman, D.G., Ringer, R.J., Wagner, T.H., Krebs, H.I., Volpe, B.T., Bever, C.T Jr., Bravata, D.M., Duncan, P.W., Corn, B.H., Maffucci, A.D., Nadeau, S.E., Conroy, S.S., Powell, J.M., Huang, G.D., & Peduzzi. P (2010). Robot-assisted therapy for long-term upper-limb impairment after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. The New England Journal of Medicine, 362(19), 1772-83.
Lum, P.S., Burgar, C.G., Shor, P.C., Majmundar, M., & Van der Loos, M. (2002). Robot-assisted movement raining compared with conventional therapy techniques for rehabilitation of upper-limb motor function after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Archives of Physical Medicine and Rehabilitation, 83, 952-9.
Lum, P.S., Burgar, C.G., Van der Loos, M., Shor, P.C., Majmundar, M., & Yap, R. (2006). MIME robotic device for upper-limb neurorehabilitation in subacute strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. subjects: a follow-up study. Journal of Rehabilitation Research and Development, 43(5), 631-42.
Luft, A.R., McCombe-Waller, S., Whittall, J., Forrester, L.W., Macko, R., Sorkin, J.D., Schulz, J.B., Goldberg, A.P., & Hanley, D.F. (2004). Repetitive bilateral arm training and motor cortex activation in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Journal of the American Medical Association, 292, 1853-61.
MacClellan, L.R., Brandham, D.D., Whitall, J., Volpe, B., Wilson, P.D., Ohlhoff, J., Meister, C., Hogan, N., Krebs, H.I., & Bever Jr, C.T. (2005). Robotic upper-limb neurorehabilitation in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients. Journal of Rehabilitation Research and Development, 6, 717-22.
Masiero, S., Armani, M., & Rosati, G. (2011). Upper-limb robot-assisted therapy in rehabilitation of acute strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients: Focused review and results of new randomized controlled trial. Journal of Rehabilitation Research and Development, 48(4), 355-66.
Masiero, S., Celia, A., Rosati, G., & Armani, M. (2007). Robotic-assisted rehabilitation of the upper limb after acute strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Archives of Physical Medicine and Rehabilitation, 88, 142-9.
Mehrholz, J., Hardrich, A., Platz, T., Kugler, J., & Pohl, M. (2012). Electromechanical and robot-assisted arm training for improving generic activitiesAs defined by the International Classification of Functioning, Disability and Health, activity is the performance of a task or action by an individual. Activity limitations are difficulties in performance of activities. These are also referred to as function.
of daily living, arm function, and arm muscle strength after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. (Review). Cochrane Database of Systematic Reviews, DIO: 10.1002/14651858.CD006876.pub3.
Nef, T., Quinter, G., Muller, R., & Riener, R. (2009). Effects of arm training with the robotic device ARMin I in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: three single cases. Neurodegenerative Disease, 6, 240-51.
Norouzi-Gheidari, N., Archambault, P.S., & Fung, J. (2012). Effects of robot-assisted therapy on strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. rehabilitation in upper limbs: systematic reviewA systematic review is a summary of available research on a given topic that compares studies based on design and methods. It summarizes the findings of each, and points out flaws or potentially confounding variables that may have been overlooked. A critical analysis of each study is done in an effort to rate the value of its stated conclusions. The research findings are then summarized, and a conclusion is provided.
and metaanalysis of the literature. Journal of Rehabilitation Research and Development, 49(4), 479-95.
Posteraro, F., Mazzoleni, S., Aliboni, S., Cesqui, B., Battaglia, A., Dario, P., & Micera, S. (2009). Robot-mediated therapy for paretic upper limb of chronic patients following neurological injury. Journal of Rehabilitation Medicine, 41, 976-80.
Rabadi, M.H., Lesser, M., & Volpe. B.T. (2008). A pilot study of activity-based therapy in the arm motor recovery post strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a randomized controlled trial. Clinical Rehabilitation, 22, 1071-82.
Reinkensmeyer, D.J., Wolbrech, E.T., Chan, V., Chou, C., Cramer, S.C., & Bobrow, J.E. (2012). Comparison of three-dimensional, assist-as-needed robotic arm-hand movement training provided with Pneu-WREX to conventional tabletop therapy after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. American Journal of Medicine and Rehabilitation, 91(11), 232-41.
Rosati, G., Gallina, P., & Masiero, S. (2007). Design, implementation and clinical tests of a wire-based robot for neurorehabilitation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 15(4), 560-9.
Song, R., Tong, K., Hu, X., & Le Li, B. (2008). Assistive control system using continuous myoelectric signal in robot-aided arm training for patients after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. IEEE Transaction on Neural Systems and Rehabilitation Engineering, 16(4), 371-9.
Staubli, P., Nef, T., Klamroth-Marganska, V., & Reiner, R. (2009). Effects of intensive arm training with the rehabilitation robot ARMin II in chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. patients: four single-cases. Journal of NeuroEngineering and Rehabilitation, 6(46), 1-10.
Stein, J., Narendran, K., McBean, J., Krebs, K., & Hughes, R. (2007). Electromyography-controlled exoskeletal upper-limb-powered orthosis for exercise training after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. American Journal of Physical Therapy and Rehabilitation, 86, 255-61.
Vergaro, E., Casadio, M, Squeri V., Giannoni, P., Morasso, P., & Sanguineri, V. (2010). Self-adaptive robot training of strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. survivors for continuous tracking movements. Journal of NeuroEngineering and Rehabilitation, 7(13), 1-12.
Volpe, B.T., Krebs, H.I., Hogan, N., Edelstein, L., Diels, C., & Aisen, M. (1999). Robot-training enhanced motor outcome in patients with strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. maintained over 3 years. Neurology, 53(8), 1874-6.
Volpe, B.T., Krebs, H.I., Hogan, N., Edelstein, L., Diels, C., & Aisen, M. (2000). A novel approach to strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. rehabilitation: Robot-aided sensorimotor stimulation. Neurology, 54(10), 1938-44.
Volpe, B.T., Lynch, D., Rykman-Berland, A., Ferraro, M., Galgano, M., Hogan, N., & Krebs, H.I. (2008). Intensive sensorimotor arm training mediated by therapist or robot improves hemiparesis in patients with chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Neurorehabilitation and Neural Repair, 22(3), 305-10.
Whitall, J., McCombe Waller, S., Silver, K.H.C., & Macko, R.F. (2000). Repetitive bilateral arm training with rhythmic auditory cueing improves motor function in chronic hemiparetic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain., 31, 2390-5.
Zollo, L., Rossini, L., Bravi, M., Magrone, G., Sterzi S., & Guglielmelli, E. (2011). Quantitative evaluation of upper-limb motor control in robot-aided rehabilitation. Medical Biological Engineering and Computing, 49, 1131-44.
Excluded Studies:
Burgar, C.G., Lum, P.S., Scremin, A.M., Garber, S.L., Van der Loos, H.F., & Kenney, D. (2011). Robot-assisted upper-limb therapy in acute rehabilitation setting following strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: Department of Veterans Affairs multisite clinical trial. Journal of Rehabilitation Research and Development, 48(4), 445-58.
Reason for exclusion: This paper compared two different robot-assisted training intensities (low and high dose) to conventional therapy where the focus of the study was intervention intensity.
Burgar, C.G., Lum, P.S., Shor, P.C., Machiel Van der Loos, H.F. (2000). Development of robots for rehabilitation therapy: the Palo Alto VA/ Stanford experience. Journal of Rehabilitation Research and Development, 37, 663–73.
Reason for exclusion: This paper summarizes preliminary results from clinical trials that are included in this review.
Daly, J.J., Hogan, N., Perepezko, E.M., Krebs, H.I., Rogers, JM., & Goyal, K.S. (2005). Response to upper-limb robotics and functional neuromuscular stimulation following strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. Journal of Rehabilitation Research and Development, 42 (6), 723-36.
Reason for exclusion: This paper compared robot-assisted training to neuromuscular stimulation. Studies where neuromuscular stimulation is used are not currently included in this StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. Engine module.
Hesse, S., Werner, C., Pohl, M., Rueckriem, S., Mehrholz, J., & Lingnau, M.L. (2005). Computerized arm training improves the motor control of the severely affected arm after strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a single-blinded randomized trial in two centers. StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain., 36(9), 1960-6.
Reason for exclusion: This paper compared robot-assisted training to functional electrical stimulation. Studies where functional electrical stimulation is used are not currently included in this StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. Engine module.
Hollenstein, C. & Cabri, C. (2011). [Zusatztherapie mit computerunterstutztem Trainingssystem im Bergleich zu ergotherapeutischer Armgruppentherapie]. Neurorehabilitation, 3(1), 40-2.
Reason for exclusion: This paper is published in German.
Hsieh, Y.W., Wu, C.Y., Liao, W.W., Lin, K.C., Wu, K.Y., & Lee, C.Y. (2011). Effects of treatment intensity in upper limb robot-assisted therapy for chronic strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.: a pilot randomized controlled trial. Neurorehabilitation and Neural Repair, 25(6), 503-11.
Reason for exclusion: This paper compared two different robot-assisted training intensities (low and high dose) to conventional therapy where the focus of the study was intervention intensity.
Johnson, M.J., Feng, X., Johnson, L.M., & Winters, J.M (2007). Potential of a suite of robot/computer-assisted motivating systems for personalized, home-based, strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. rehabilitation. Journal of NeuroEngineering and Rehabilitation, 5(6), 1-17.
Reason for exclusion: This is a feasibility study quantifying immediate motor performance and muscle activation across devices.
Mayr, A., Kofler, M., & Saltuari, L. (2008). ARMOR: an electromechanical robot for upper limb training following strokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain.. A prospective randomized controlled pilot study. Handchirurgie, Mikrochirurgie, Plastische Chirurgie, 40(1), 66-73.
Reason for exclusion: This paper compared robot-assisted training to functional electrical stimulation. Studies where functional electrical stimulation is used are not currently included in this StrokeAlso called a "brain attack" and happens when brain cells die because of inadequate blood flow. 20% of cases are a hemorrhage in the brain caused by a rupture or leakage from a blood vessel. 80% of cases are also know as a "schemic stroke", or the formation of a blood clot in a vessel supplying blood to the brain. Engine module.